Exam Technique - Last-Minute Golden Tip
The simplest, last-minute exam tip of all time
Here is the simplest Exam Technique tip ever:
Don’t fold the exam paper back on itself
Students typically fold the paper back to reduce it to A4 size, and to focus on just one page. Don’t do this!
Often, questions straddle more than one page. These will appear opposite sides of the fold. Keep the paper open, and you will be able to see all the information at once. Something from an earlier part of the question may well be vital for answering the last part. Don’t hide it from view!

More posts with exam tips:














Exam Technique - Simplify the Question
Make the Question Simpler
Let’s get rid of everything that isn’t on the spec. We will need these words later when writing the answer out, but we do NOT need them while we work out what the question is really about.
To be brutally honest, most students who get stuck on exam questions do so because they don’t understand the content deeply enough. There is no magical exam technique that can make up for that.
However, there are certainly some things you can do to make exams easier.
Here’s a great exam tip for anyone who gets overwhelmed when they see a question like the one below:
Overwhelming scary question:

What is Dihydrofolate Reductase?? That’s not on the spec! 😩😭
Don’t panic if you don’t recognise words in a question - if it’s not on the spec, you are not being tested on your knowledge about it.
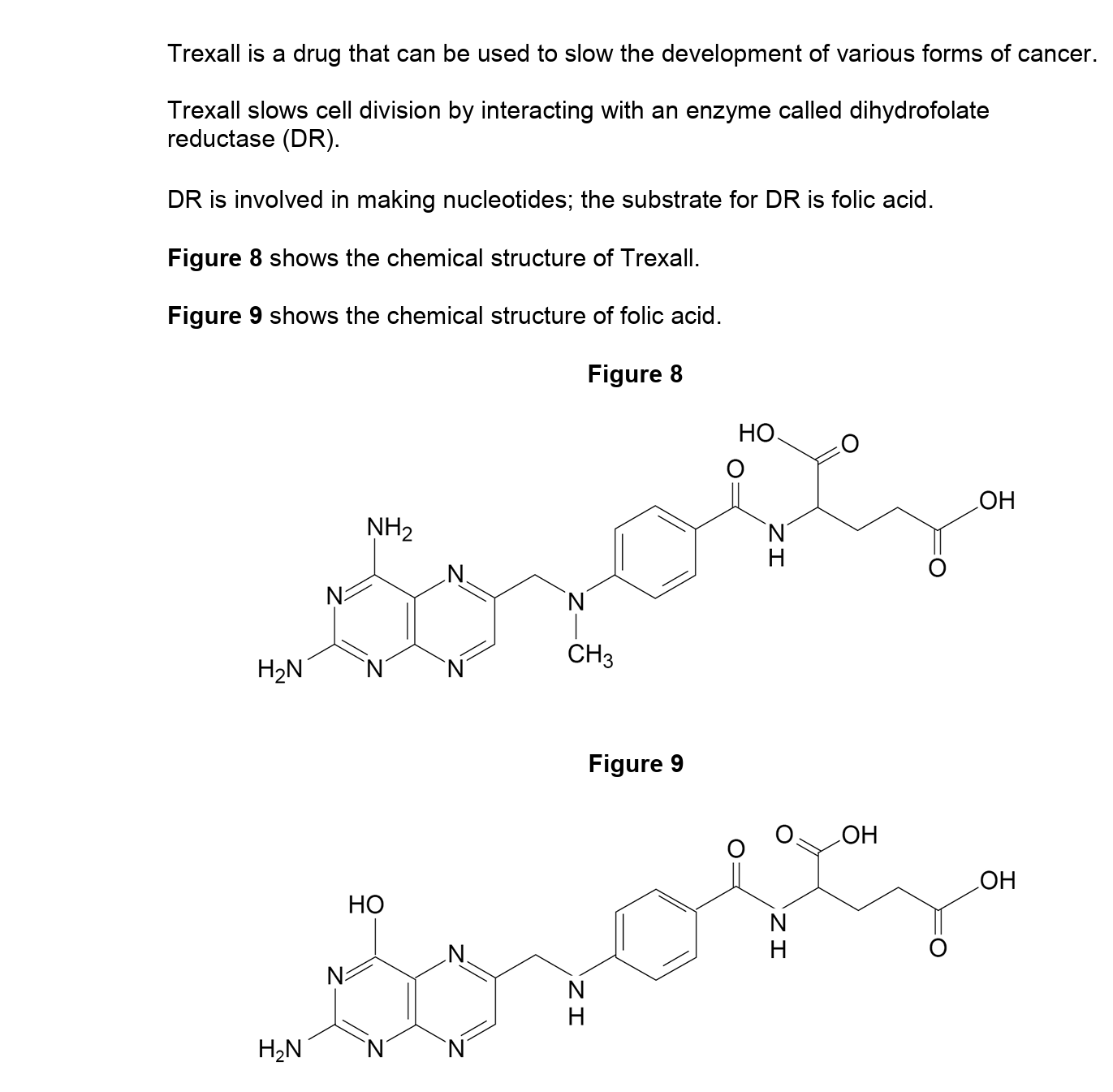
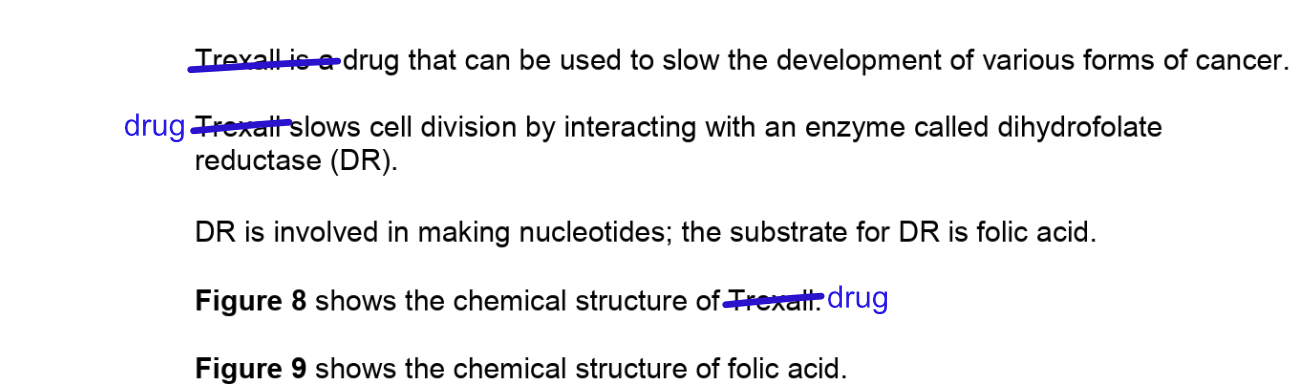
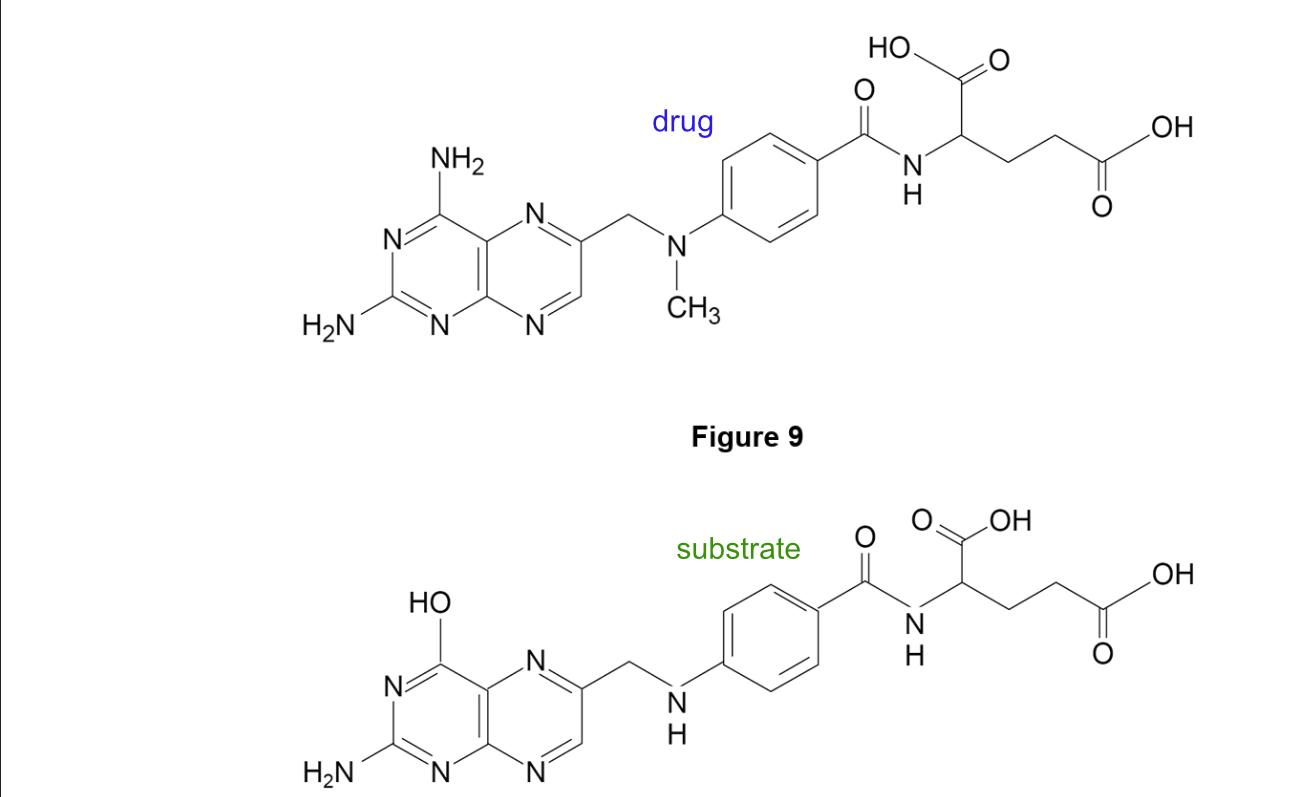
That means that this question is not about dihydrofolate reductase, nor about Trexall
So what is it about?
Look for the familiar words and concepts. Focus on those, not on the weird jargon names of the example organisms/molecules/drugs that you have never seen before. They are just examples, the important thing are the general concepts.
Make the Question Simpler
Let’s get rid of everything that isn’t on the spec. We will need these words later when writing the answer out, but we do NOT need them while we work out what the question is really about.
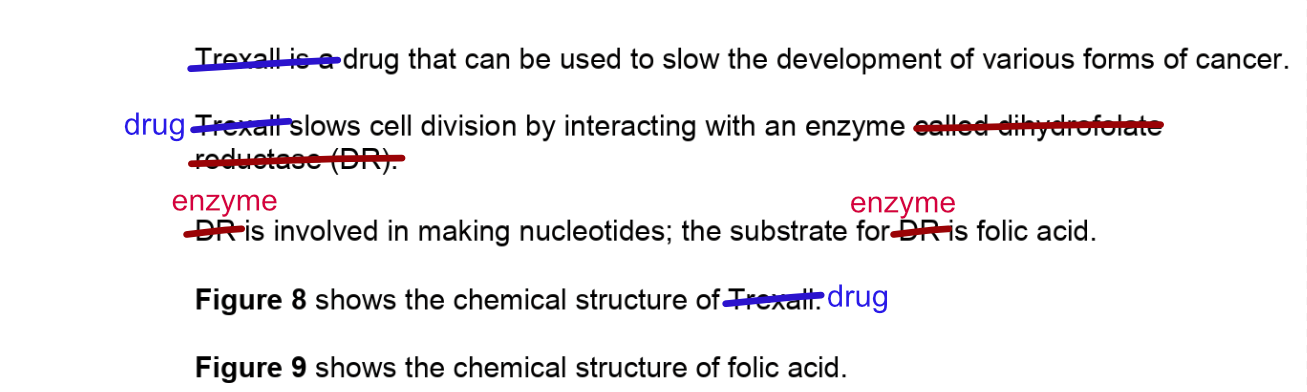
First, let’s replace “Trexall” with “Drug”. Trexall isn’t on the spec so it’s just an example of a drug. The name isn’t important.
Do the same for the enzyme. You don’t need to remember that DR = dihydrofolate reductase while you’re working out the general, on-spec concept of the question. If you stick all that in your brain you’ll have less capacity for thinking about the important things.
And then the same for the substrate (Folic Acid is not on the spec, the concept of substrates is).
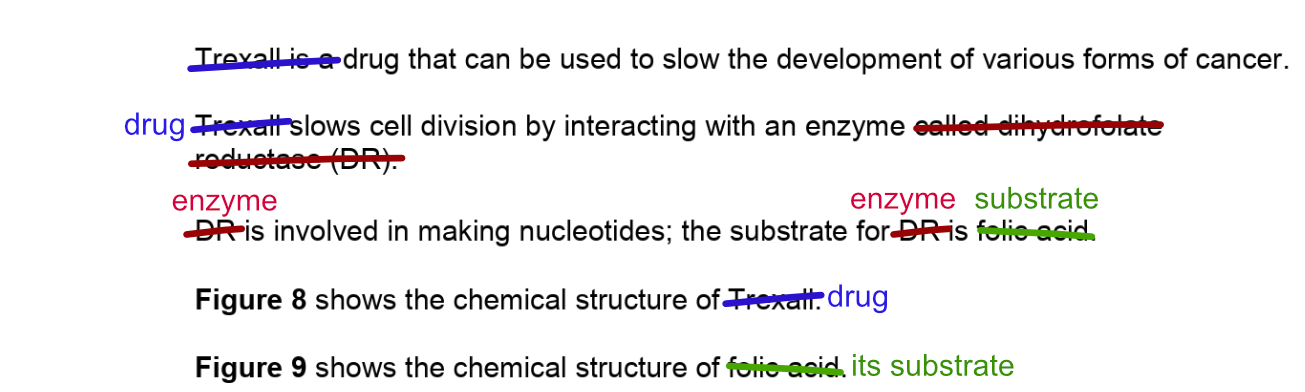
In summary: cross out the names of things that are not on the spec, and repace with generic words.
Hm, that sentence “the substrate for enzyme is substrate” is a bit pointless. So we can cut all that.
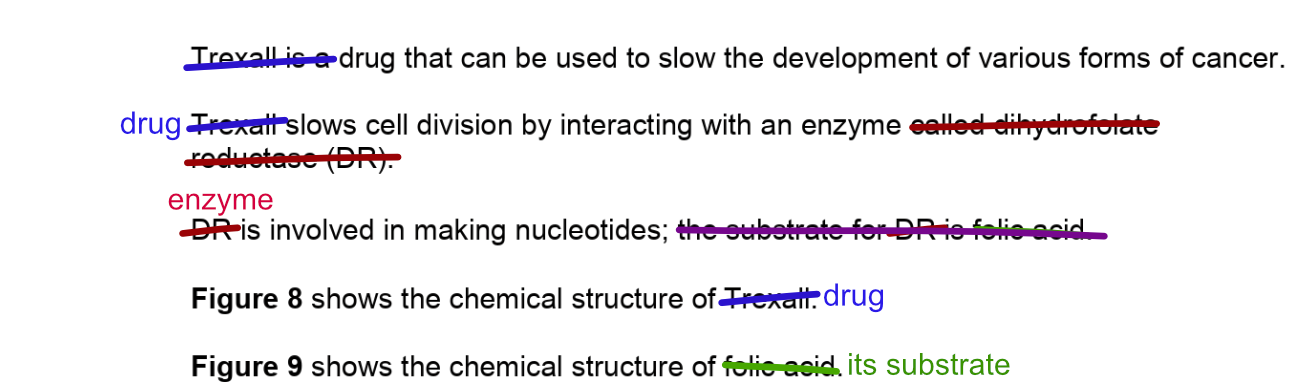
This is hopefully looking a little bit less overwhelming now.
The other thing we can do is to directly label the figures, so you don’t have to look up and down to remember which is which. This is for any type of figure - if it’s a graph, you would label the axes.
That helps a bit, but those molecular structures are still pretty scary stuff.
But remember: these molecules are not on the spec - so they are just examples. Two molecules, either of which might have had pretty much any structure.
What is the very first, most obvious and basic thing that you noticed about them when you looked at them together?
The Question Itself

Interesting, nothing about cancer in the question. We know that cancer involves fast-dividing cells, so a drug that slows cell division might help, but it doesn’t want you to talk about cancer (for this question at least). So that top sentence in the background info isn’t actually required either.
Also notice that it the question says “use the information provided” - this is a clue that everything you need is in the background information. They were never expecting you to already know anything about Trexall or dihydrofolate reductase.
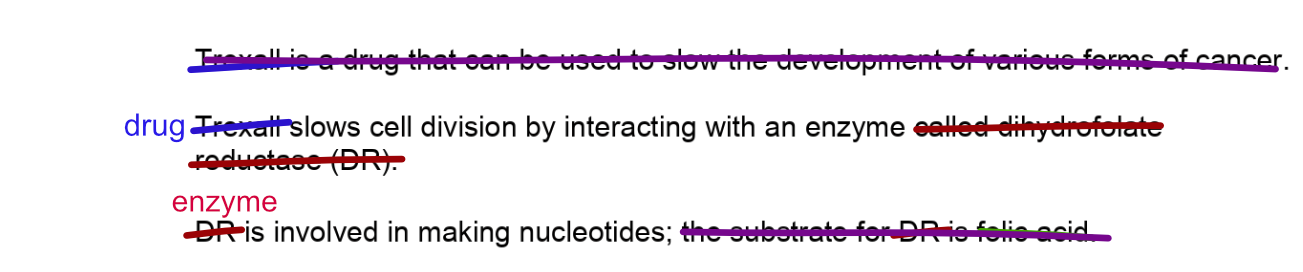
The question has been simplified down to this:
▪ A drug slows cell division by interacting with an enzyme
▪ The enzyme is involved in making nucleotides
▪ The drug and the enzyme substrate look very similar
Suggest how the drug slows cell division
Can you work out the answer now? Give it a go before reading on.
Working Out the Answer
There are two important things you need to realise - firstly the mechanism of action of the drug, and secondly why its action slows cell division. Both of these rely on you knowing concepts from the spec.
1. The Mechanism of Action of the Drug
What have you learned about different ways in which drugs might work? How might a drug interact with an enzyme? How might a drug with a structure very similar to the substrate interact with an enzyme? How might that affect the enzyme?
2. Why does this Action Slow Cell Division?
The enzyme is involved in making nucleotides. Nucleotides are on the spec. What are they used for in the cell? How is this connected to cell division?
Writing Out the Answer
When you write out your answer, it’s really important to remember to reverse the simplification process and use the correct names of the drug, enzyme, and substrate!
Give it a go now if you haven’t already - write out the answer you would give. Then scroll down to check it against the answers & markscheme. Don’t jump ahead; practicing writing answers to exam questions is really important for learning. I promise nobody will see if you mess it up.
Answer & Markscheme
There are many ways to explain the answer to get the marks, here’s just one example:
Trexall has a molecular structure very similar to folic acid, which is the substrate of the enzyme DR. This suggests that Trexall acts as a competitive inhibitor by binding the enzyme’s active site. This action prevents folic acid from binding, reducing the number of enzyme-substrate complexes. As the enzyme is involved in nucleotide synthesis, Trexall slows the rate of that process. Nucleotides are required for DNA replication, which is required for cell division. Trexall slows cell division by reducing the number that are available to a point where their availability is a limiting factor.
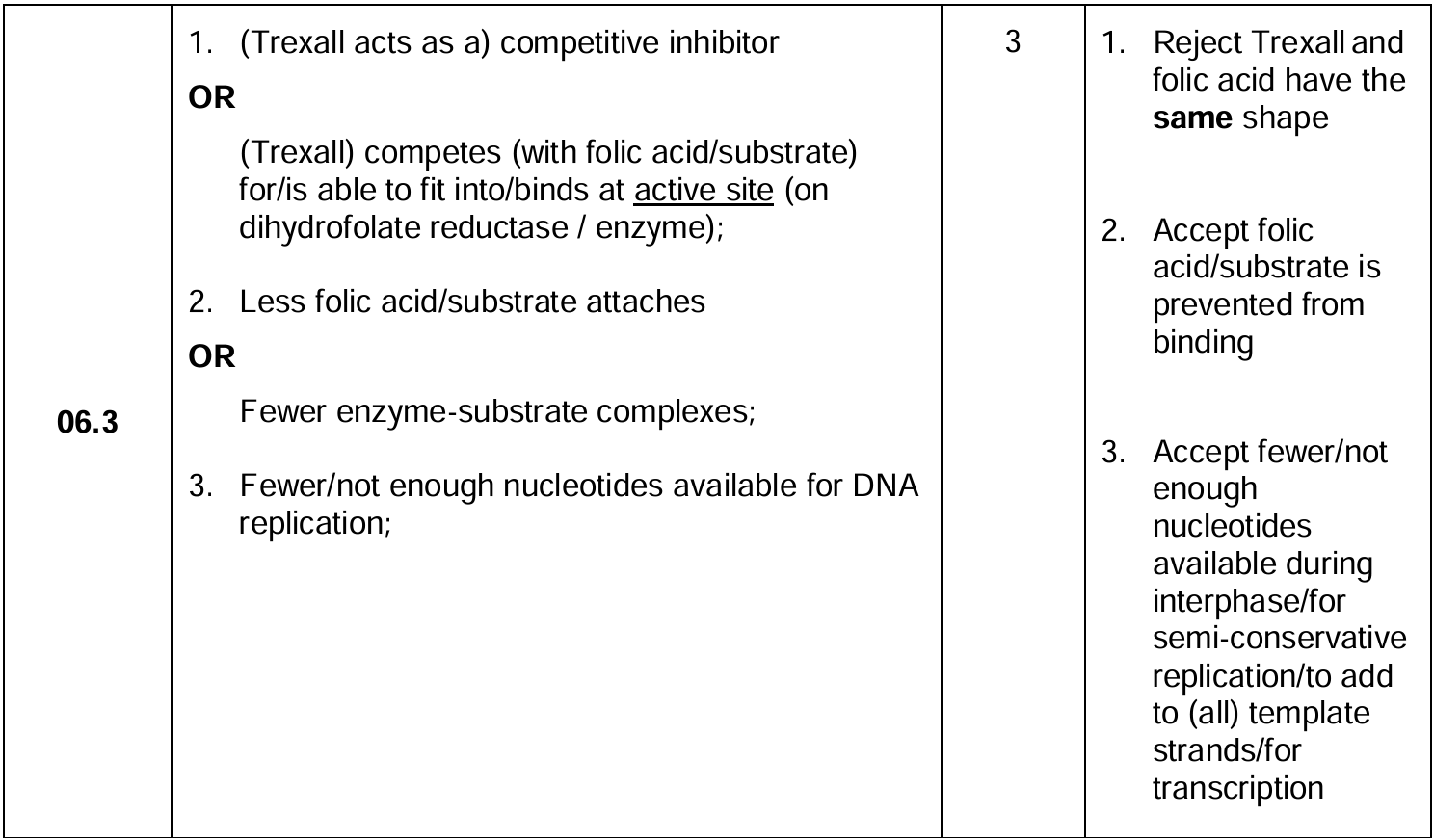
Can you see where the marks came from? And did you get all three?
Top tip: there’s no point in trying to remember answers to exam questions - the questions in your exam will be different! Instead, focus on noticing things like the level of technical language and detail that are required, and how these compared to your answer.
A Quick Recap to Finish..
If you feel overwhelmed by the amount of information in an exam question, you can simplify the question by removing specific names of things that are not on the spec - which you are not being examined on - and replacing these by the general concepts that you are being examined on. Just remember to use specific language in your actual written answer.
The full Exam Tip collection:
Give yourself a moment to think about the previous post before surging forward - maybe go make some tea. But here is more food for thought.

Preparing for A level Biology: what can I do in the summer
What can you best do over the summer to help transition to A level Biology? (It's probably not what you're thinking.)
Tips and information to help with the transition from GCSE to A level.

Aiming for Success
Pressure on students seem to grow every year, with more and more students looking to do work over the summer to prepare for starting A level Biology in the autumn term. It’s true that A level Biology is a challenge, and there are certainly things you can do that will help your studies. This article gives advice on what you can best do to hit the ground running when you start your A level course.
One thing I don’t recommend is to ask a tutor to teach you A level content before you start. All this will do is interfere with your teacher’s work and make the classroom less interesting as there will be no surprises. That’s not a great way to build motivation for the long term. It’s much better to encounter new topics in the classroom, and use tutoring to check/deepen understanding and correct misconceptions.
The best things you can do over the summer are things that will (1) help consolidate your prior knowledge and understanding, and (2) create anchor points for you to learn/remember new knowledge.
You’re not going to like the first, but the second might be just what you need right now.
Consolidate Prior Knowledge
How did you do at GCSE?
A level biology builds upon concepts that you studied for GCSE. Having these solid in your mind will help massively when you are introduced to new materials. If you know you are a bit wobbly on some topics, watch out because that will make it difficult for you to understand the A level material - you’ll effectively need to learn both levels of content at the same time. And that’s a real challenge. Mastering the GCSE material will mean you can use it with little mental effort while grappling with the more-complex A level concepts.
Ok so it might feel weird to back go over GCSE content when the exams are done and dusted, but you’re going to need all that stuff again in your A level course. Maybe go back through it in August in the run-up to starting your A-level studies, and drill down into any areas where you feel like you’ve just memorised it without any real understanding.
Look at this comparison of the spec for GCSE and A level Cell Structure:
AQA A level Cell Structure
The structure of eukaryotic cells, restricted to the structure and function of:
cell-surface membrane
nucleus (containing chromosomes, consisting of protein-bound, linear DNA, and one or more nucleoli)
mitochondria
chloroplasts (in plants and algae)
Golgi apparatus and Golgi vesicles
lysosomes (a membrane-bound organelle that releases hydrolytic enzymes)
ribosomes
rough endoplasmic reticulum and smooth endoplasmic reticulum
cell wall (in plants, algae and fungi)
cell vacuole (in plants).
In complex multicellular organisms, eukaryotic cells become specialised for specific functions. Specialised cells are organised into tissues, tissues into organs and organs into systems.
Students should be able to apply their knowledge of these features in explaining adaptations of eukaryotic cells.
AQA GCSE Cell Structure
Students should be able to explain how the main sub-cellular structures, including the nucleus, cell membranes, mitochondria, chloroplasts in plant cells and plasmids in bacterial cells are related to their functions.
Most animal cells have the following parts:
a nucleus
cytoplasm
a cell membrane
mitochondria
ribosomes.
In addition to the parts found in animal cells, plant cells often have:
chloroplasts
a permanent vacuole filled with cell sap.
Plant and algal cells also have a cell wall made of cellulose, which strengthens the cell.
Recognise, draw and interpret images of cells.
Students should be able to use estimations and explain what they should be used to judge the relative size or area of sub-cellular structures.
You can see that there is a lot of overlap - the GCSE content is used as a foundation for learning more. Because you already know something about organelles and their general functions, you can build additional understanding by adding to this prior knowledge. Learning everything from scratch would be really hard! That’s why you need GCSE qualifications to enter the course - your GCSE knowledge will act as a springboard. But how good that springboard is might vary across topics.
You’ll also need to know how to calculate areas and volumes, and to read graphs and understand how averages can be used to understand data. How did you do at GCSE maths?
A person with strong GCSE Biology and Maths will find it much easier to learn A level Biology than someone with a poor grade in combined science. Not because they’re cleverer (whatever that means), but simply because they’re starting from a better place.
What to do: if you know you’re weak on some parts of GCSE, take a look back over those areas and make sure you have a strong foundation for learning more. You’re going to have it re-learn it at some point, and it’s easier to do it while you’re not also grappling with higher-level concepts that won’t make sense without that prior knowledge.
Stretch your Literacy

A level Biology involves a lot of complex vocabulary and comprehension of texts. Written language is very different from spoken language, so if you usually consume informal, spoken media it may be more difficult for you to follow biology texts.
Reading any long-form, professionally written texts will help stretch your literacy and get you used to the vocabulary and sentence structures used in formal writing. It would be ideal to read a pop-sci biology book on a subject that interests you, but reading any books with formal-stye writing, on just about any topic, would be a great boost.
Literacy is a huge factor in student success, and especially anyone with lower grades in GCSE English would benefit from getting more used to reading long-form written-language texts. If you’re struggling to understand the language before you even start to grapple with the biological concepts, the course will be extra-difficult for you.
What to do: find a well-written blog, or book, or other long-form media that interest you and get used to reading in an engaged, thoughtful way. Put your phone aside and practice focusing on the text and its meaning, thinking about how it links to your own interests and life.
Enrich your mind
The human brain is unable to remember facts in isolation. This is why memory experts need to use mnemonic tricks. It’s much, MUCH easier to remember things if they relate to things we already value, our life experiences, our self-image, our emotions, or our prior knowledge.
This makes A level Biology more difficult for students who been unable to travel, or have perhaps focused purely on classroom study. In biology you will encounter many examples of animals and environments that are well-known to some students, but new to others.
A student who has visited a rainforest will find it easier to learn and remember new information about rainforests not only because they might already know some things, but also because they can link new information to their prior experience.
Students with little experience may also get tripped up by organisms that are used as ‘well known’ examples to illustrate points. Some students don’t know what cows eat, or that dolphins are not fish, or that bats are mammals. Well-meaning teachers can confuse students with less-broad life experience by assuming knowledge that just isn’t there.
I’m not suggesting you don’t know what cows eat, or that you visit a rainforest (although do if you can - they’re awesome). But you absolutely can enrich your mind with different experiences and stories and images that will serve you well as anchors for future learning.

Visit different environments
If you can visit a zoo, or an aquarium - perfect! Take your time to really observe the animals. Build strong memories by taking notice of the smells and sounds around you. Read the labels. Talk to your friends about what you see, relating your observations to other things you already know about. Then, later in the course, when your teacher talks about the neck-bones in a giraffe, you can stick that information on to your memory of the giraffe in the zoo. It sounds silly but seriously, it’s like a cheat code for learning.
Maybe you can find a volunteer opportunity in the summer helping with conservation work. This can give you a real connection to the environment you’re working in, and an understanding of what it’s like to work in the field that will help you better imagine, and remember, the field studies described in your course.
Or, just visit the park. Go for a walk by a river. Notice the small organisms around you. The weeds in the cracks. Stop to observe insects. What can you smell? Notice how different animals are hanging out in different environments. In what ways do these environments vary? Stick your hand in a river, feel the texture of the leaves of a tree and notice how the top and bottom surfaces are different. Listen to the wind and birdsong, talk, build emotional and sensory memories that will provide strong anchors for future learning. Touch grass.
What to do: visit different environments, exploring with all your senses while observing and discussing the organisms you discover.

Go on a virtual adventure
Documentaries and films can take you to a vast variety of environments that you wouldn’t be able to visit in person.
Check out BBC Nature documentaries and fall into the emotional stories they tell of individual animals. Imagine how the animal feels, its challenges, abilities and basic drives. Get a really broad view of the diversity of environments and organisms on Earth and the delicate interactions. When you later learn about some A level concept, you will suddenly think “oh, wait, it’s like that thing I saw!” and suddenly it’ll all make sense and be easy to remember.
If you don’t live in the UK, especially if your local environment is very different, how about watching some programmes about, or set in, British farmland. Find out what cows eat! Examples from farming and agriculture are found throughout the course and will be less accessible to you if they are unfamiliar.
What to do: immerse yourself in rich visuals, music and stories of environment and organisations from around the planet.

The best part about building these rich memories is that it won’t burn you out. You can enjoy the experience without having to do difficult analytic thinking, trying to force information into your brain, or recalling complex information.
Let’s face it, if you’ve just finished your exams then more academic study might not be what you need right now.

So in summary …
Broaden your mind and lay the foundational knowledge that you will need to engage with A level Biology concepts. In this way you can set yourself up for an easier time in the classroom in September - and throughout the whole course.
Article by Jenny Shipway. If you liked it, click ❤️Like below to help others find useful articles.
How to Revise A Level Biology: A Simple Trick - Use Your Words
A simple but effective trick to boost your learning and revision. You just need a little buddy.

A guest blog from Dr Jenny Shipway, who studied biochemistry at university and now works in science communication and education training.
Find the full set of “How to Revise” articles here
The Lazy Brain
Brains are great at taking sneaky short-cuts to avoid thinking too hard, especially when they’re feeling tired. If you get stuck on something while revising, it might be for this reason.
Words are Powerful
Words not only help us communicate, but also help us organise our thoughts. By forcing things into words, we can prevent our brains from taking short cuts, and force them to think things through properly.
Many problems can be solved simply by stating the problem out loud. How many times have you asked someone for help but, as you are describing the problem you realise what the answer is? By describing the problem step by step, it’s suddenly obvious where you were going wrong.
As a bonus, when you take the effort to put things into your own words this forces the thoughts through your brain in a way that means you are more likely to remember it in future.
Your best study buddy is already in the room

Can you explain Mitosis to Mr Pokey?
Research shows that much of what people learn in schools comes from talking with their teachers and classmates. But what if you’re alone? Don’t despair, your study buddy does not have to be human, or even alive.
As you study, you could explain concepts out loud to:
Your pet
A beloved soft toy
A smiley face drawn on your finger
A picture of someone you love or respect
Pretty much anything with two googly eyes stuck onto it
I don’t know what the research says about giving your buddy a name, but I would imagine this would help too.
Keep Your Language On Track
For best effect:
Speak in complete sentences rather than letting your thoughts jump around. If you need to repeat yourself to do this, then do so (your study buddy won’t mind). Making yourself repeat the same idea again but more clearly is really helpful.
Keep your language scientific and appropriate to the level of study where possible.
Don’t let your brain take short-cuts by using unprecise language or skipping through ideas. Speak slowly and deliberately, like you really are trying to explain something to someone who doesn’t already know it.
By repetitively speaking biology jargon words out loud, you will be much more likely to remember them in future. And by using them in complete, meaningful sentences, you will be telling your brain that they are useful things to recall and flagging them up as things worth remembering in future.
It’s important that you’re not just repeating sentences you read elsewhere, the key is to produce new sentences that serve a purpose in explaining something to your study buddy.
If this post has been helpful, please like ❤️ below and share with your friends.

Key Concept: Averages, Range, and Standard Deviation, with A level Biology Past-Paper Questions
You need to know some maths for A level Biology. This includes knowing how to interpret averages (mean, median and mode), ranges, and standard deviations to work out whether an experiment can be said to have shown an effect or not. Master this early on and it will not help you with exam questions, but also make it easier for you to learn the bits of the course that are explained using these statistical methods.
You need to know some maths for A level Biology. This includes knowing how to interpret averages (mean, median and mode), ranges, and standard deviations to work out whether an experiment can be said to have shown an effect or not. Master this early on and it will not help you with exam questions, but also make it easier for you to learn the bits of the course that are explained using these statistical methods.

Why does Biology need so much data?

Maybe the guy at the back is just big for his age?
Researchers often want to compare two or more things. Which species of frog is heavier? Which type of soil grows taller plants? At what temperature do these bacteria divide fastest? At which pH are fish most active?
The biological world is complicated, so multiple, repeated measurements are usually required.
There are three main reasons for taking multiple measurements:
Measurement errors. It’s hard to take measurements in the real world. Even if you re-measure the exact same thing, and even if you use a well-calibrated tool, you might get a slightly different result each time. Maybe you can’t hold the tool still enough, or you can’t read it clearly, or the thing you’re measuring moves. These are precision errors.
Individual variation. If you want to ask a general question about a whole population, eg “do robins sing more than blackbirds” then you need to measure data from more than two individuals. If you only use two, you might randomly pick outliers; maybe you get a particularly perky robin, or a lazy/sick blackbird. Similarly, if you sample a small area of a larger region, you may not pick a representative area.
Uncontrolled variables.There will nearly always be variable-influencing factors that you’re not aware of, or unable to control. Maybe there are changing sounds or smells in the environment, subtle changes in light, or in the birds’ blood-sugar levels. These can affect individual measurements in unpredictable ways.
All of these things can affect the value you record, making any one single measurement unreliable. So researchers normally end up collecting large sets of measurements. In this way they can get a much better idea of what’s really going on.
Why does Biology need Statistical techniques?
Plotting lots of repeated measurements for different datasets on the same graph can create a confusing mess. Also, “the data look different to me” isn’t good enough for science.
Reducing each dataset to just two or three values makes it much easier to compare. In fact, it’s so simple that such data can be understood even without a graph, so values are often presented very simply in a table.
Calculating Averages in Biology
There are three types of average: mean, median, and mode. They all reduce the data set to one single number.
This is useful for comparisons. For example, if you let a frog jump ten times, measuring the length of every jump, you can calculate their average jump length. You can then compare that single number to the average jump length from another frog to find out which jumps further.
Calculating the Mean
The most important type of average for A level Biology is the mean. It’s also what most people are talking about when they say “average” in everyday life.
To find the mean, add up all the numbers, then divide by how many numbers there were. You end up with just one number.
Here’s an example dataset:
| Set 1 | 3 | 4 | 5 | 5 | 5 | 6 | 6 | 6 | 7 | 8 | total = 55 / n = 10 / mean = 5.5 |
| Set 1 | 3 | 4 | 5 | 5 | 5 | 6 | 6 | 6 | 7 | 48 | total = 95 / n = 10 / mean = 9.5 |
| Set 1 | 3 | 4 | 5 | 5 | 5 | 6 | 6 | 6 | 7 | 48 | central number(s) = 5 and 6 / median = 5.5 |
| Set 1 | 1 | 3 | 5 | 5 | 5 | 5 | 6 | 6 | 7 | 48 | mode = 5 |
| Set 1 | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 50 | mean = 50 / median = 50 / mode = 50 | ||
| Set 2 | 25 | 30 | 35 | 40 | 50 | 50 | 60 | 65 | 70 | 75 | mean = 50 / median = 50 / mode = 50 | ||
| Set 3 | 1 | 2 | 3 | 4 | 50 | 50 | 96 | 97 | 98 | 99 | mean = 50 / median = 50 / mode = 50 |
The averages are the same! By themselves, averages only tell you one small part of the story.
What is Range / why is it useful
One of the big differences betwen the datasets above is the range of numbers that appear.
The range is the range-of-values that appear, from the lowest to the highest.
| Set 1 | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 50 | lowest value = 50 / highest value = 50 / range = 50 to 50 | ||
| Set 2 | 25 | 30 | 35 | 40 | 45 | 55 | 60 | 65 | 70 | 75 | lowest value = 25 / highest value = 75 / range = 25 to 75 | ||
| Set 3 | 1 | 2 | 3 | 4 | 50 | 50 | 96 | 97 | 98 | 99 | lowest value = 1 / highest value = 99 / range = 1 to 99 |
Set 1 has a range of 50 to 50. So you can reasonably predict that the next measurement would likely be 50 too
Set 2 and Set 3 have wider ranges. There are a wider range of possible values that might be measured, so it’s harder to predict what the next measurement might be.
A wide range might indicate that your measurement technique is very unprecise, or that there is a wide natural variation in the thing you are measuring, or that there is another factor affecting your measurements.
But a wide range might also just mean there were one and two weird outliers in the data. So you need to be careful when using this value. Here is a set with one odd measurement, which might be due to a measurement error.
| Set 4 | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 50 | 90 | lowest value = 50 / highest value = 90 / range = 50 to 90 |
| Set 1 | 25 | 42 | 48 | 50 | 50 | 50 | 50 | 52 | 58 | 75 | values clustered around mean = low standard deviation | ||
| Set 2 | 25 | 30 | 35 | 40 | 45 | 55 | 60 | 65 | 70 | 75 | values spread out away from mean = high standard deviation |
To understand Standard Deviation, think about a situation where you have made very many measurements, so that you have multiple measurements at each possible value. Now plot these on a graph (see below). In biology, you usually see that the graph forms a bell shape. This is called a “Normal distribution”.
Normal distributions are symmetrical, so the mean, mode, and median are all the same, appearing at the centre of the graph (mean, median, and mode = 16 in this example). In normal distributions, most measurements are near the average, so there is a peak in the middle of the graph.
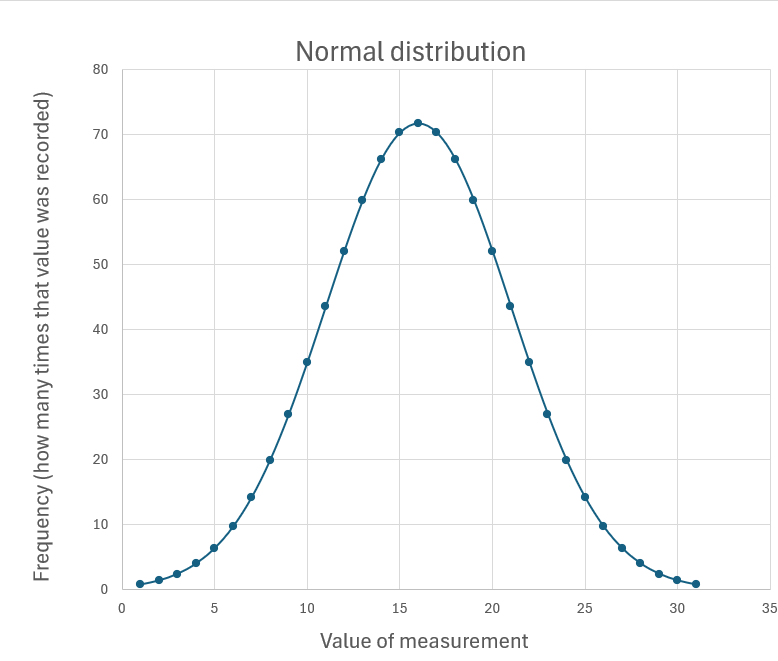
(Sometimes, you’ll find a curve is skewed a bit to one side. This separates out the mode, median and mean values. But for our purposes, I’m going to stick to thinking about the symmetrical graph.)
How wide the curve is matters a lot, because it affects how much two sets of data overlap. Compare these two examples below. Both have one set of data where the mean is 14 (plotted in orange), and another set where the mean is 20 (plotted in blue).
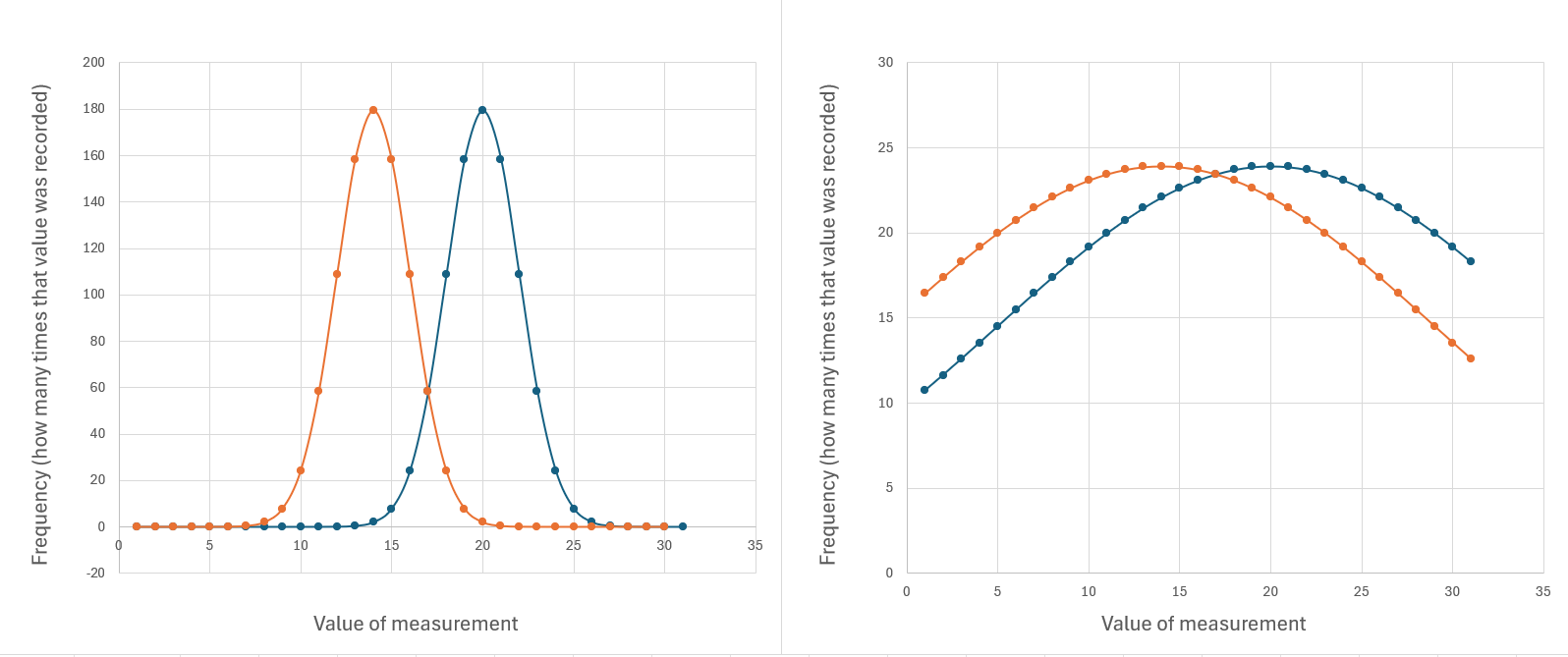
There is the same amount of data in both graphs, and the averages haven’t changed. But there is a lot less overlap between the two datasets in the example to the left. The data on the right is a lot more spread out away from the average values.
When datasets overlap a lot, you need to be very careful that you definitely have enough data to be sure their means really are different. If you have a small data set with a lot of variation, then adding extra measurements can make a big difference to the mean.
What is Standard Deviation
Standard Deviation tells you how widely the data is spread out in a normal distribution. Its symbol is sigma, “σ”.
You’re very unlikely to be asked to calculate standard deviation in an exam, and it takes a while to explain so I’m not going to go through it here (don’t worry they’d give you the equation if you did have to do this).
But you do need to know what it tells you.
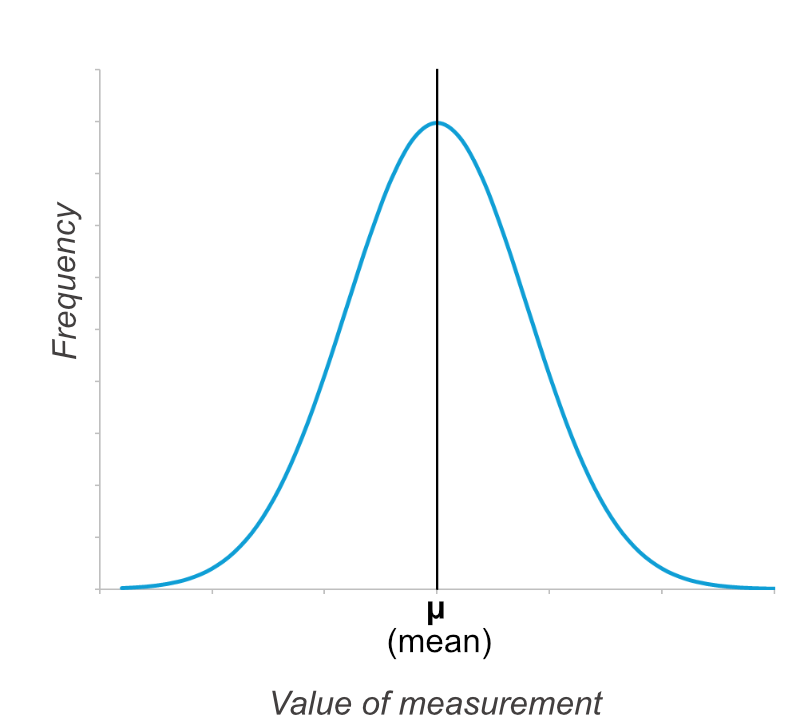
Here is the basic normal distribution graph again. The graph is symmetrical and the mean (μ) is in the centre.
Now here is the same graph, but two more values are marked on the x-axis, shown by orange lines. These are the value of the mean minus one standard deviation (μ-σ), and the value of the mean plus one standard deviation (μ+σ).
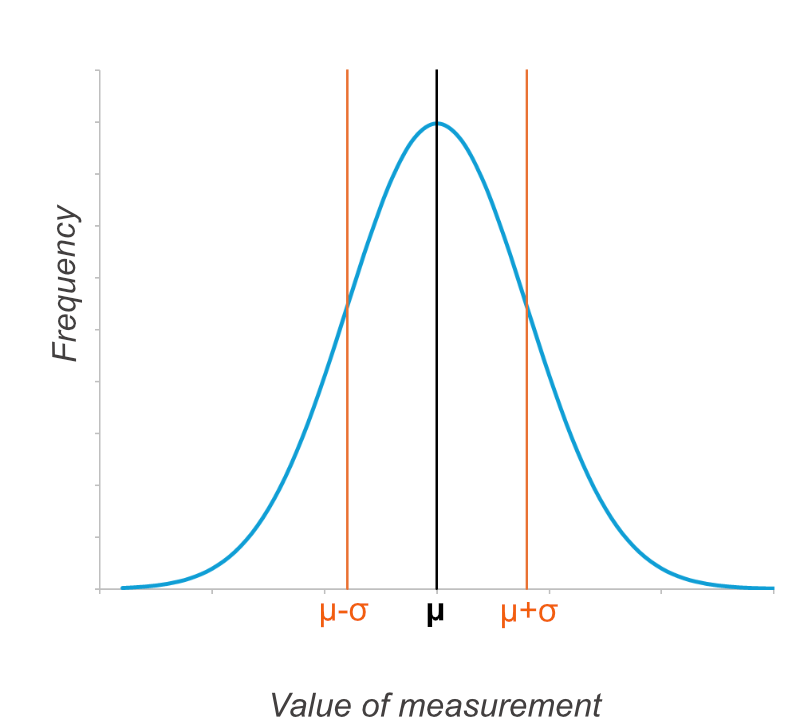
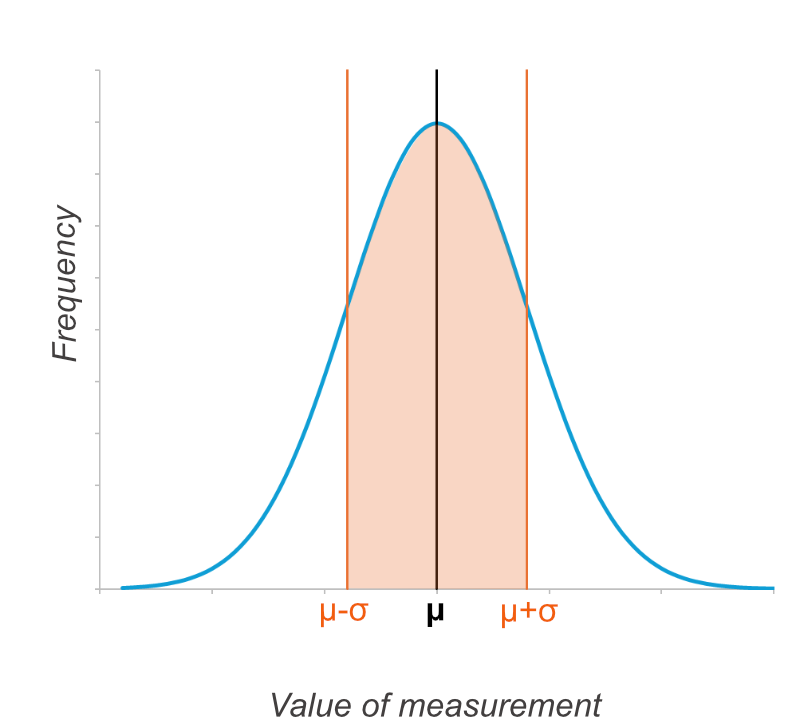
If you colour in the bit of the graph that is within one standard deviation of the mean (from μ-σ to μ+σ), then on any normal distribution, 68.27% of the data points will lie within this area. You don’t need to remember that percentage, but remember it is always the same.
This means that if the standard deviation is a small number, you know most of the data points are close to the mean. This gives you more confidence that the mean is a useful value for comparison.
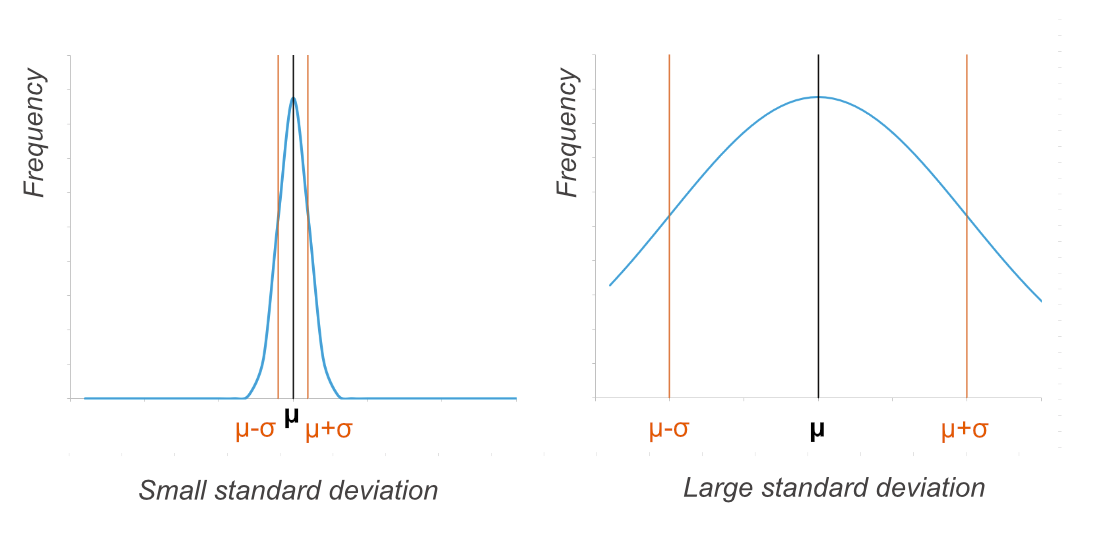
The graphs below have the same X-axis. Both are normal distributions with the same mean. But the one on the left has a small standard deviation, and the one on the right has a high standard deviation. (Some of the data from the right-hand graph falls outside the values shown on the graph.)
How to tell if there is a significant difference between values using the mean and standard deviation
!! Ok so this is the important bit we’ve been building up to !!
In a normal distribution, most of the data (68.27%) falls within one standard deviation of the mean. This is the area between μ-σ and μ+σ.
To work out whether it’s just chance that the means are different, or whether it’s a real effect, you need to check whether this area overlaps bewteen the two sets of data.
If the areas between μ-σ and μ+σ overlap, the difference is not considered significant.
There are different ways of presenting the data.
Standard Deviations Using Numbers - example
An example:
Set 1: mean (μ) = 50, standard deviation (σ) = 8
Set 2: mean (μ) = 40, standard deviation (σ) = 3
Are these sets of data significantly different? Look at the areas between μ-σ and μ+σ
Set 1: μ-σ = 42 and μ+σ = 58
Set 2: μ-σ = 37 and μ+σ = 43
Do these areas overlap? Yes they do (both include 42-43). So you can not consider the two data sets significantly different.
(Also worth knowing: nearly all the data (95.45%) falls within two standard deviations (between μ-2σ and μ+2σ) - so if these two areas don’t overlap you can be even more sure the two sets of data really are different.)
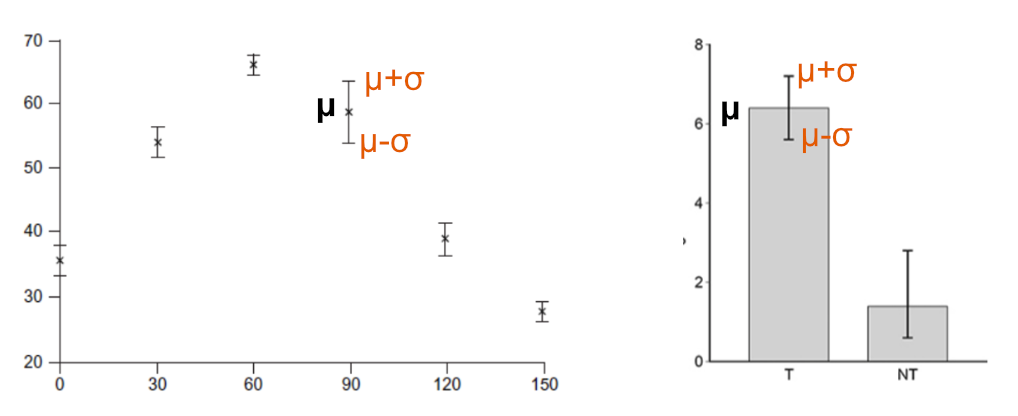
Standard Deviations Plotted on Graphs - example
On graphs, the mean is plotted as usual, with a dot or column. Extra lines extend out to show the area from μ-σ to μ+σ. This can make it more obvious whether areas overlap or not (unless they are super close in which case numbers are more useful).
Standard Deviation Exam Past Papers
Example Exam Question 5
Question 5 answers found at the bottom of this web page
Understanding Standard Deviations from Graphs
Example Exam Question 6
Question 6 answers found at the bottom of this web page
Example Exam Question 7
Question 7 answers found at the bottom of this web page
Graphs and Tables in A level Biology
If you’re not confident with questions that include graphs and tables, see the recent blog post “How to Approach A level Biology Graph and Table Questions: Tips and Exam Question Pack”, which offers more useful tips for navigating them during exams, and more exam questions to practice with.
Answers to example exam questions
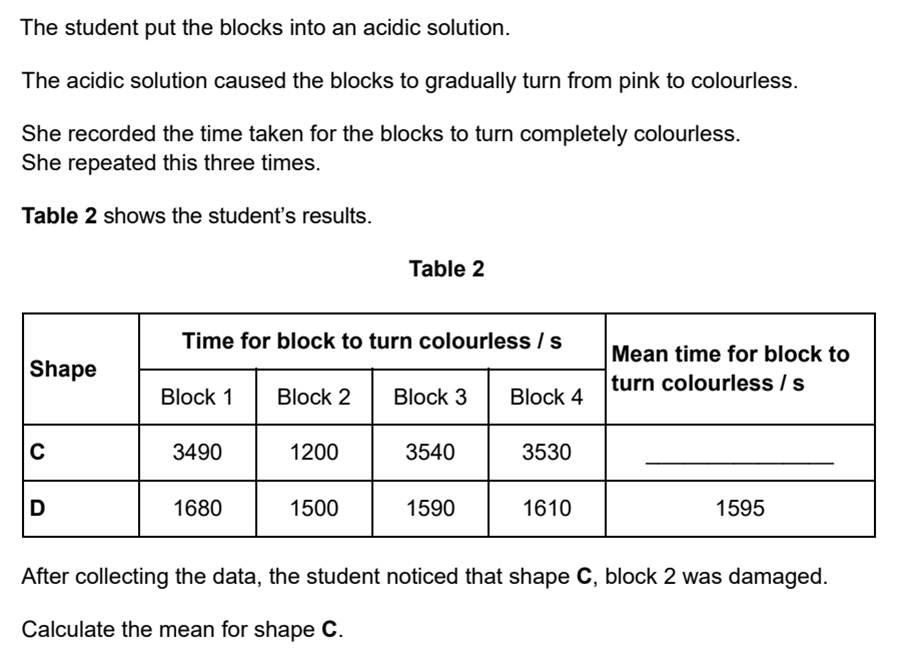
The data for the damaged block should be ignored. The mean for shape C is 3520 seconds
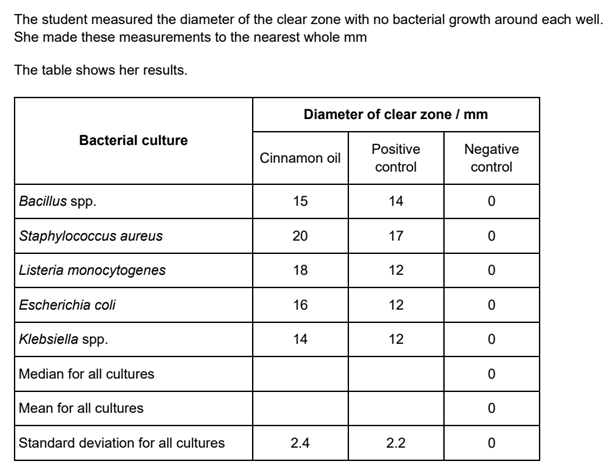
Cinnamon Oil median = 16, mean = 17 ….. and ….. Postive Control median = 12, median = 13
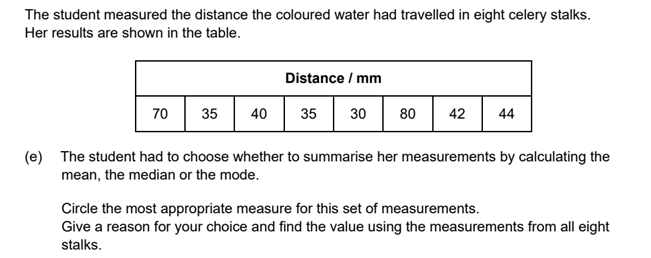
Median = 41. This avoids the outliers affecting the value as would happen if you used the mean. And the sample size is too small to use the mode (there are no repeated values)
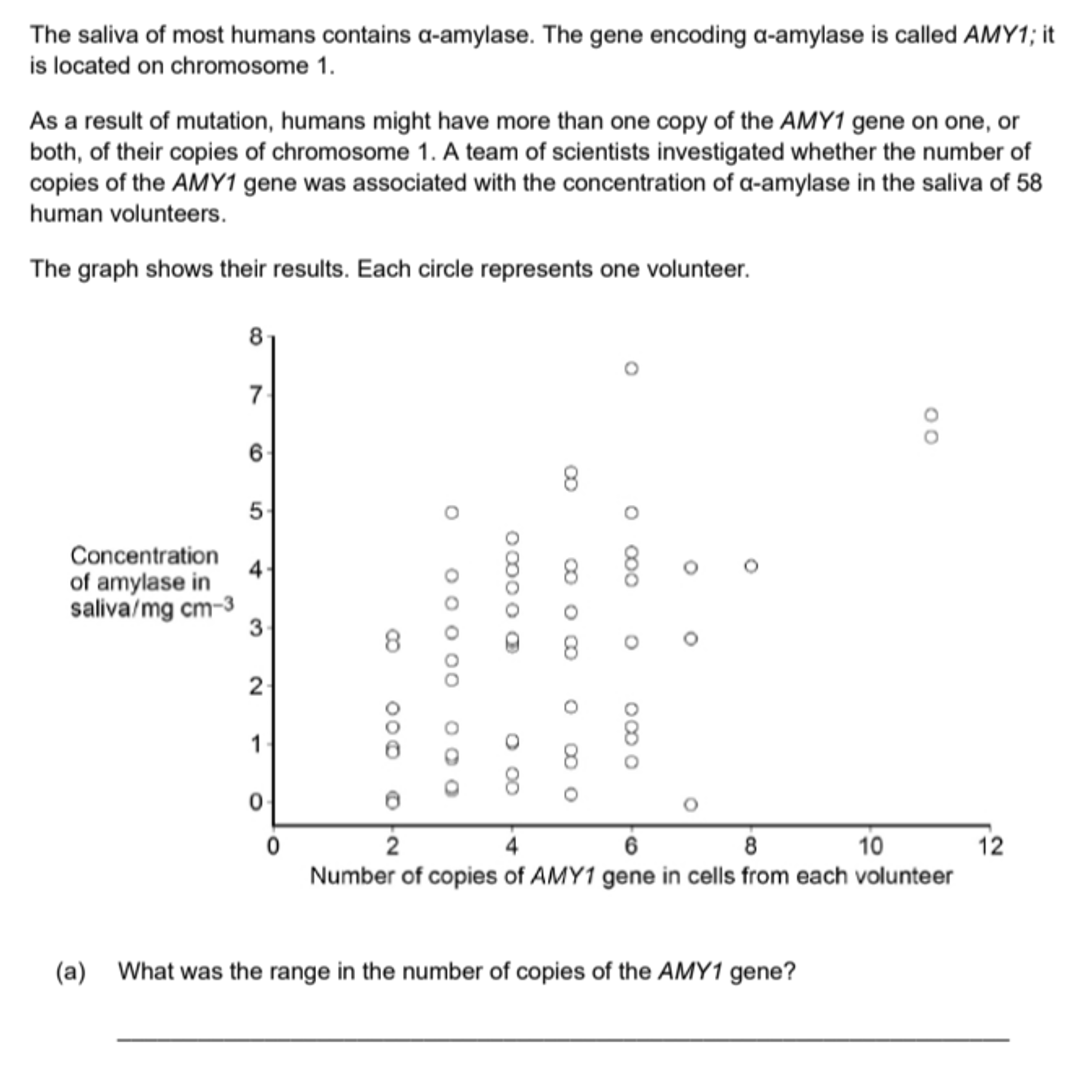
The range is 2 to 11
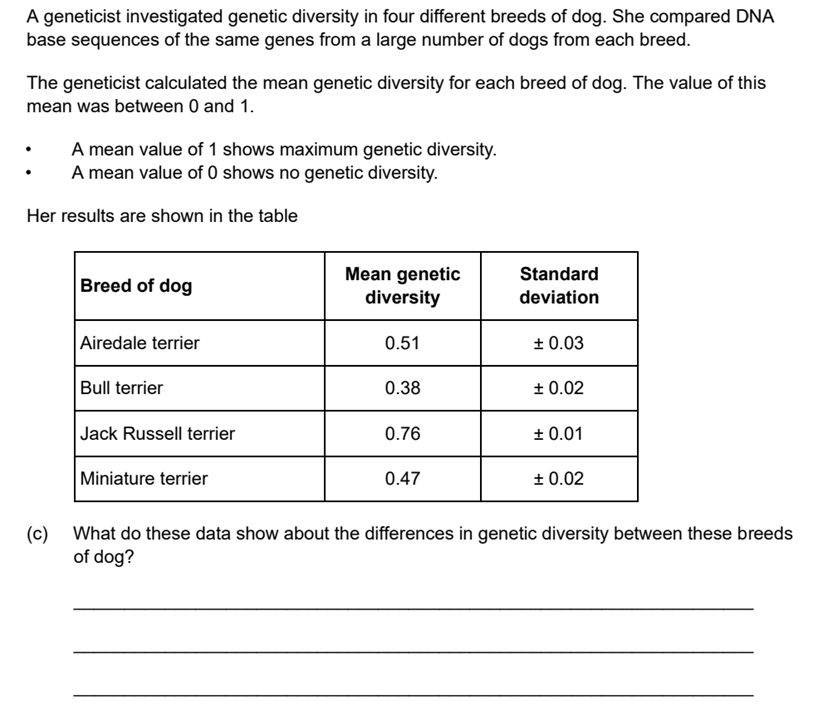
Bull terrier genetic diversity is significantly the smallest of the breeds shown, meaning it the most inbred. Jack Russell genetic diversity is significantly the greatest. The genetic diversity of Miniature terrier and Airedale terriers are similar with no significant difference between the two.
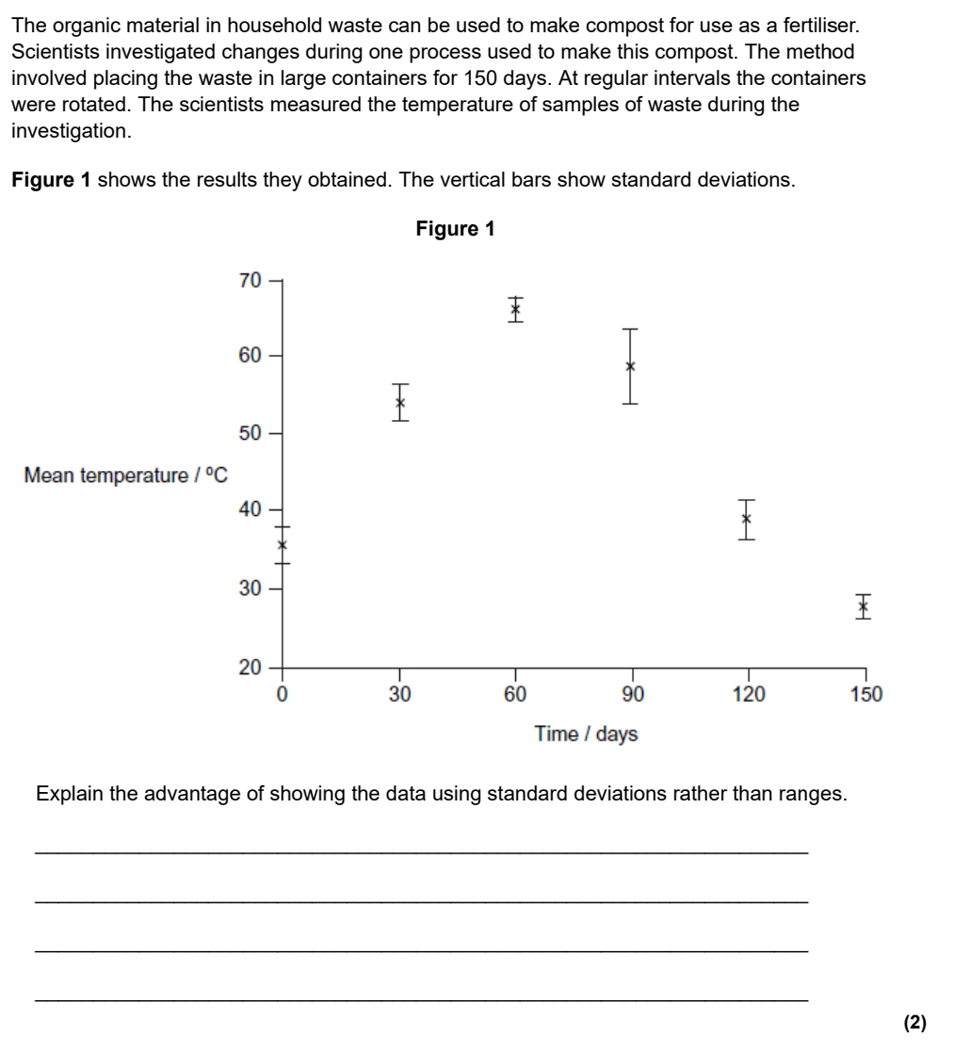
Standard deviation is spread of data around the mean; using standard deviation reduces effect of anomalies/ outliers; standard deviationcan be used to determine if (the difference in results is) significant/not significant/due to chance /not due to chance
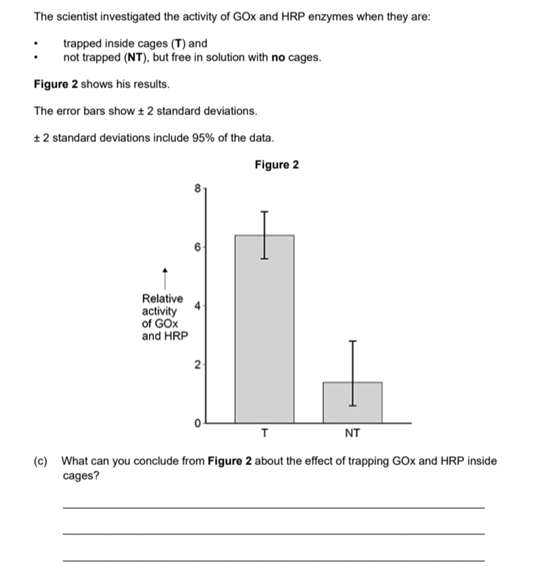
Trapping increases enzyme/GOx/HRP activity; the difference/increase is significant (it is unlikely to be due to chance as the standard deviations do not overlap)
Photosynthesis - OCR A MCQs Self Marking Quiz
Self-marking multiple choice quiz for Photosynthesis. Using OCR A past paper exam questions.
Amino acids and Proteins - OCR A Self Marking Quiz
Self-marking multiple choice quiz for Proteins. Using OCR A past paper exam questions.
Quizzes are really important for retention !
Food Tests and Chromatography- OCR A Multiple Choice Questions - Self marking Quiz
Self-marking multiple choice quiz for Food Tests and Chromatography. Using OCR A past paper exam questions.
Quizzing is really helpful for retention of knowledge
Phospholipids, Lipids and Cholesterol - OCR A Multiple Choice Questions - Self marking Quiz
Self-marking multiple choice quiz for Phospholipids, Lipids, and Cholesterol. Using OCR A past paper exam questions.
Quizzing is really helpful for retention of knowledge
Carbohydrates, Ions and Elements - OCR A Multiple Choice Questions
Self-marking multiple choice quiz for Carbohydrates, Ions and Elements. Using OCR A past paper exam questions.

Booking now: OCR A Y13, Tuesdays 6:30pm from September 2026 to June 2027
Weekly Group Masterclasses for OCR A Y13
Raise your exam grade with question focused masterclasses from a highly experienced A level Biology teacher.
Every week we go through a different topic from the specification and look at how to apply the content to OCR A exam questions. I show how to understand commonly occurring questions and how to answer them.

Weekly Group Masterclasses for OCR A Y13
Raise your exam grade with question focused masterclasses from a highly experienced A level Biology teacher.
Every week we go through a different topic from the specification and look at how to apply the content to OCR A exam questions. I show how to understand commonly occurring questions and how to answer them.
“Outstanding A-level Biology tutoring! Patient, engaging, and highly personalised—even in group classes, it feels one-to-one. Recorded sessions, all questions answered, and every student involved. Our daughter jumped a grade and achieved an A and a place to study Medicine at University” - Google reviews 2025
During the lesson students use an interactive whiteboard to write answers to exam questions which (only) I can see and comment on. Students can ask questions at any time but are not required to speak on camera to the group. The classes run in focus mode on zoom - so I can see every student, but they are not visible to the rest of the class.
Students can stream a recording after their lesson for revision and note taking.
I teach using evidence-based educational theory. With decades of A level Biology class and one-to-one teaching experience, I am very aware of the misconceptions and misunderstandings that cause students to unnecessarily struggle, and of the mistakes that can lead to dropped marks in exams.
By correcting these issues, students not only do better in exams but also learn to enjoy studying Biology.
The typical class size is 6-12 students. No payment is taken in advance. The classes are £45 per lesson. The card you use to reserve your place is charged after the lesson.
OCR Biology A Y13 Schedule (2026–2027) Time: Tuesdays at 6:30 PM Notes: Closed for Christmas (Dec 22 & 29); Includes sessions during Easter.
| Month | Date | Spec Ref | Topic Focus |
|---|---|---|---|
| September 2026 | 15 Sep | 5.2.1 (a–d) | Photosynthesis – chloroplasts, pigments, light-dependent stage |
| 22 Sep | 5.2.1 (e–h) | Photosynthesis – Calvin cycle and limiting factors | |
| 29 Sep | 5.1.1 (a–d) | Communication and Homeostasis | |
| October 2026 | 06 Oct | 5.2.2 (d–g) | Respiration – Part 1 (Krebs cycle, oxidative phosphorylation) |
| 13 Oct | 5.2.2 (a–c) | Respiration – Part 2 (Glycolysis, anaerobic, RQ) | |
| 20 Oct | 5.1.4 (a–c) | Hormonal Communication – Part 1 | |
| 27 Oct | 5.1.4 (d–e) | Hormonal Communication – Part 2 | |
| November 2026 | 03 Nov | 5.1.2 (a–b) | Excretion and the liver (incl. diabetes) |
| 10 Nov | 5.1.2 (c–d) | Kidneys – Part 1 (Structure and nephron function) | |
| 17 Nov | 5.1.2 (d–f) | Kidneys – Part 2 (Osmoregulation and dialysis) | |
| 24 Nov | 5.1.3 (a–d) | Nerves – Part 1 (Resting and action potentials) | |
| December 2026 | 01 Dec | 5.1.3 (e–g) | Nerves – Part 2 (Synapses and transmission) |
| 08 Dec | 5.1.5 (a–c) | Animal responses (Brain, reflexes, heart rate control) | |
| 15 Dec | 5.1.5 (d) | Meiosis recap, monohybrid, codominance, sex linkage | |
| 22 Dec | — | No Lesson (Christmas) | |
| 29 Dec | — | No Lesson (Christmas) | |
| January 2027 | 05 Jan | 5.1.5 (e–f) | Inheritance: Dihybrid, autosomal linkage, epistasis |
| 12 Jan | 6.1.2 (c–d) | Chi-squared and t-test | |
| 19 Jan | 6.3.1 (a–d) | Succession, distribution, and abundance | |
| 26 Jan | 5.1.5 (l) | Muscle contraction | |
| February 2027 | 02 Feb | 6.1.1 (a–c) | Cellular Control – mutations and gene regulation |
| 09 Feb | Revision | Revision lesson on the whole of Module 5 | |
| 16 Feb | 6.1.3 (a–b) | Manipulating Genomes – DNA & gene sequencing | |
| 23 Feb | 6.1.3 (c–e) | DNA profiling, PCR, and gene analysis | |
| March 2027 | 02 Mar | 6.1.2 (e–f) | Evolution and Hardy-Weinberg |
| 09 Mar | 6.1.2 (g–h) | Speciation and artificial selection | |
| 16 Mar | 6.1.3 (f–g) | Gene therapy and cloning | |
| 23 Mar | 6.1.3 (h) | Genetic engineering | |
| 30 Mar | 5.1.5 (g–j) | Plant responses – Part 1 (Easter Session) | |
| April 2027 | 06 Apr | 6.3.2 (a–b) | Populations and sustainability (Easter Session) |
| 13 Apr | 6.3.2 (c–e) | Conservation, preservation, and management | |
| 20 Apr | 6.3.1 (e) | The nitrogen cycle | |
| 27 Apr | 6.3.3 (a–b) | Biotechnology – microorganisms | |
| May 2027 | 04 May | 5.1.5 (k) | Plant responses – Part 2 |
| 11 May | 6.3.1 (f–h) | Ecosystems and biomass transfer | |
| 18 May | Revision | Revision lesson - Plant transport | |
| 25 May | Final | Synoptic Links and Exam Paper Practice |
Cell Ultrastructure, Prokaryotes, Cytoskeleton Questions OCR A
Self-marking multiple choice quiz for Cell Ultrastructure, Ions, and Elements. Using OCR A past paper exam questions.
Booking now: AQA Y13 A level Biology Group Class - from Sept 2026 to June 2027
Weekly Group classes - for AQA Y13 A level BIology
Raise your exam grade with question focused masterclasses from a highly experienced A level Biology teacher.
Every week we go through a different topic from the specification and look at how to apply the content to exam questions. I show how to understand commonly occurring questions and how to answer them.
Weekly Group classes - for AQA Y13 A level BIology
Raise your exam grade with question focused masterclasses from a highly experienced A level Biology teacher.
Every week we go through a different topic from the specification and look at how to apply the content to exam questions. I show how to understand commonly occurring questions and how to answer them.
“Outstanding A-level Biology tutoring! Patient, engaging, and highly personalised—even in group classes, it feels one-to-one. Recorded sessions, all questions answered, and every student involved. Our daughter jumped a grade and achieved an A and a place to study Medicine at University” - Google reviews 2025
During the lesson students use an interactive whiteboard to write answers to exam questions which (only) I can see and comment on. Students can ask questions at any time but are not required to speak on camera to the group.
The classes run in focus mode on zoom - so I can see every student, but they are not visible to the rest of the class.
Students can stream a recording of every lesson for revision and note taking.
I teach using evidence-based educational theory. With decades of A level Biology class and one-to-one teaching experience, I am very aware of the misconceptions and misunderstandings that cause students to unnecessarily struggle, and of the mistakes that can lead to dropped marks in exams.
By correcting these issues, students not only do better in exams but also learn to enjoy studying Biology.
The typical class size is 6-12 students. No payment is taken in advance. The classes are £45 per lesson. The card you use to reserve your place is charged after the lesson.
AQA Biology Y13 Schedule (2026–2027) Time: Wednesdays at 6:30 PM Notes: Includes sessions during Easter break; closed for Christmas (Dec 23 & 30).
| Month | Date | Spec Ref | Topic Focus |
|---|---|---|---|
| September 2026 | 09 Sep | 3.4.5 | Species and taxonomy |
| 16 Sep | 3.4.6 | Biodiversity within a community | |
| 23 Sep | 3.4.7 | Investigating diversity | |
| 30 Sep | 3.5.1 | Photosynthesis – Part 1 | |
| October 2026 | 07 Oct | 3.5.1 | Photosynthesis – Part 2 |
| 14 Oct | 3.6.1.1 | Survival and response | |
| 21 Oct | 3.5.2 | Respiration – Part 1 | |
| 28 Oct | 3.5.3 | Energy and ecosystems | |
| November 2026 | 04 Nov | 3.5.2 | Respiration – Part 2 |
| 11 Nov | 3.5.4 | Nutrient cycles | |
| 18 Nov | 3.6.1.2 | Receptors | |
| 25 Nov | 3.6.1.3 | Control of heart rate | |
| December 2026 | 02 Dec | 3.6.2.1 | Nerve impulses (neurones, resting & action potentials) |
| 09 Dec | 3.6.2.2 | Synaptic transmission (summation, inhibitory, drugs) | |
| 16 Dec | 3.6.4.1 | Principles of homeostasis and negative feedback | |
| 23 Dec | — | No Lesson (Christmas) | |
| 30 Dec | — | No Lesson (Christmas) | |
| January 2027 | 06 Jan | 3.6.3 | Skeletal muscles |
| 13 Jan | 3.6.4.2 | Control of blood glucose concentration and diabetes | |
| 20 Jan | 3.6.4.3 | Control of blood water potential – Part 1 | |
| 27 Jan | 3.6.4.3 | Control of blood water potential – Part 2 | |
| February 2027 | 03 Feb | 3.7.1 | Inheritance – Part 1 |
| 10 Feb | Revision | Revision lesson of questions on 3.5 and 3.6 | |
| 17 Feb | 3.7.1 | Inheritance – Part 2 | |
| 24 Feb | 3.7.2 | Populations and Hardy-Weinberg | |
| March 2027 | 03 Mar | 3.7.3 | Evolution may lead to speciation |
| 10 Mar | 3.7.4 | Populations in ecosystems (including succession) | |
| 17 Mar | 3.8.1 | Alteration of DNA sequences and effects on proteins | |
| 24 Mar | 3.8.2.1-2 | Non-coding DNA / Regulation of transcription & translation | |
| 31 Mar | 3.8.2.3, 3.8.3 | Gene expression and cancer / Using genome projects | |
| April 2027 | 07 Apr | 3.8.4.1 | Recombinant DNA technology (Easter Session) |
| 14 Apr | 3.8.5, 3.8.6 | Probes and DNA fingerprinting (Easter Session) | |
| 21 Apr | Stats | Stats tests, P values, SD, range, and averages | |
| 28 Apr | Maths | Maths Questions and Magnification | |
| May 2027 | 05 May | Eval | Evaluation Questions |
| 12 May | Exam | Extended Response Question Practice | |
| 19 May | Review | Synoptic Links and Paper 3 Prep | |
| 26 May | Final | Last-minute Q&A and Exam Technique |
Another "Suggest" AQA exam question walk through
Example 2: Q3 Paper 2 2023
This next question is more complex, and there are two ‘suggest’ questions.
But first - I always recommend you don’t read the actual questions until you’ve looked at the background information, graph etc. Doing this will help you avoid getting overwhelmed and jumping to mistaken conclusions (which is very common in exam situations!).
So let’s keep the questions for later. First make sense of this:
Here is another example of a “Suggest” question from a past paper.
Find the main “Suggest” article and first example question here
Example 2: Q3 Paper 2 2023
This next question is more complex, and there are two ‘suggest’ questions.
But first - I always recommend you don’t read the actual questions until you’ve looked at the background information, graph etc. Doing this will help you avoid getting overwhelmed and jumping to mistaken conclusions (which is very common in exam situations!).
So let’s keep the questions for later. First make sense of this:
1. Don’t panic!
This question is going to challenge your working memory by throwing lots of information at you all at once. Tackle it bit by bit to make sense of what’s going on.
2. Use your knowledge to make sense of the background information:
There are tomatoes, a “mycorrhizal species’, and different water conditions.
You know that mycorrhizae are fungi (3.5.4)
You know that plants need the correct amount of water in order to grow (GCSE)
You can understand the experiment – including identifying the independent, dependent, and controlled variables. (8.3)
You can understand the data – what is the graph is showing? (6.4)
Top tip: Write “IV” and “DV” on the paper to identify the Independent and Dependent variables.
Water availability = IV
Whether mycorrhizae were added to the soil = IV
The mean mass of tomatoes = DV
…. What is the graph showing?
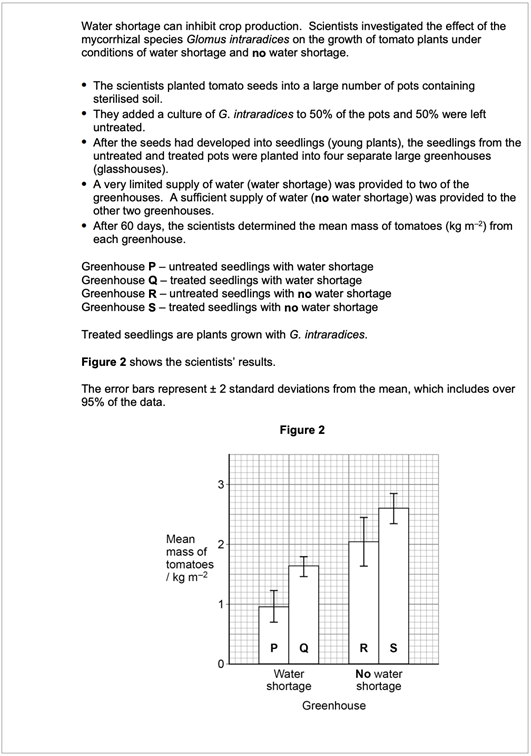
· The pair of bars on the left of the graph compare the yield of tomatoes from plants grown in conditions of water shortage.
o The bar on the far left is for plants grown in soil that did not have mycorrhize added. The other is for plants in soil that did have mycorrhizae added.
o The results show a significant difference between the yield of tomatoes for these two groups of plants. The plants with mycorrhizae yielded more tomatos.
· The pair of bars on the right compare plants that did not experience water shortage.
o Again, the bar on the left is without mycorrhizae, and that on the right is with mycorrhizae.
o The results show no significant difference between the yield of tomatoes from these two groups of plants.
Got that? Ok now you’re ready to look at the questions. How would you approach these?
3. Answer questions in order:
The first part of the question (not shown) is about phosphorous cycles, so you will already be thinking about content from 3.5.4 (Nutrient Cycles).
4. Check the Command Word:
‘Suggest’.
5. Understand the question:
These questions are quite straightforward.
6. Think about relevant information from the spec
You know that mycorrhizae facilitate the uptake of water and inorganic ions by plants. (3.5.4)
You know that there are a variety of living organisms in soil, and that these are in competition (3.7.4)
ou have identified the fertiliser concentration as a controlled variable (8.3)
7. How many marks are there available?
Each question has two reasons for two marks; one mark per reason. Make them good ones!
8. So, what are your answers?
There are a variety of different ways to get the marks, allowing you to play to your strengths. Give it a go before looking at the makr scheme below.
..
..
..
..
..
..
..
..
..
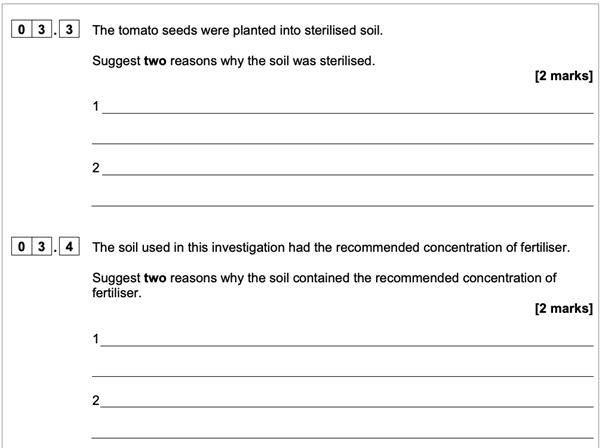
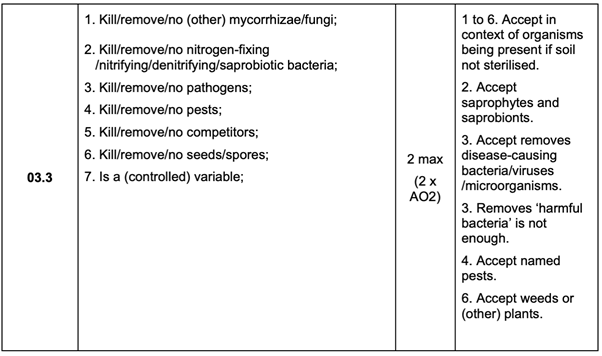
Q3 Paper 2 2023 Q3.3 – mark scheme
Did you get the marks?
Paper 2 2023 Q3.3 – example answers
Good answer examples, which would win marks:
✅ to ensure that there are no other fungi growing in the soil
✅ to remove any seeds in the soil so that other plants don’t grow and consume the nutrients and water
✅ to ensure that there are no pathogens in the soil that can infect the tomato plants
Poor answers that would not get the mark – can you identify where they’ve gone wrong?
❌ To remove harmful bacteria
❌ To kill everything living in the soil so it doesn’t interfere with the experiment
❌ to make sure that conditions are ideal for growing tomato plants
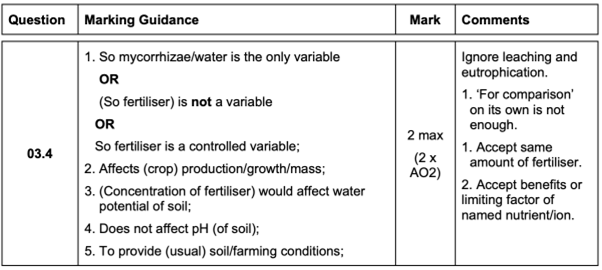
Q3 Paper 2 2023 Q3.4 - markscheme
Paper 2 2023 Q3.4 – example answers
Good answer examples, which would win marks:
✅ The investigation is on the effect of water shortage so the concentration of fertiliser should be a control variable
✅ The concentration of fertiliser will affect the growth of the plant so the recommended amount should be used to get the best crop
✅ Fertilisers can affect the water potential of the soil which may impact how water is absorbed by the roots
Poor answers that would not get the mark – can you identify where they’ve gone wrong?
❌ Without fertiliser the tomatoes won’t grow
❌ So that the soil doesn’t affect the size of the tomatoes
❌ So that the tomatoes can be compare
Article by Natalie Vlachakis (an ex-teacher who also worked for AQA) & Jenny Shipway
How to answer "Suggest" questions in AQA A level Biology
Command words are important! Step by step guide to how to approach and answer “Suggest” questions for top marks in AQA A level Biology.
Article by Natalie Vlachakis (an ex-teacher who also worked for AQA) & Jenny Shipway
Command Words: What do you Suggest?
There are many ways that examiners can ask an A-level Biology question. They might ask you to describe the structure of DNA. Or to explain the importance of the xylem being kept open as a continuous tube.
In exam questions, words like ‘describe’, ‘explain’ (and ‘suggest’) are known as command words. Always pay attention to command words because they tell you what type of knowledge or skill is being tested, and how you should approach the question.
So - when you get a question that asks you to ‘suggest’ something, what exactly does it want from you?
‘Suggest’ Questions
‘Suggest’ questions are usually asking you to use your biology knowledge and understanding to make sense of, and build upon, information about an unfamiliar organism and/or experiment.
Using unfamiliar contexts is a way for examiners to check that you really understand the content; rather than just having memorised set phrases and information.
You aren’t expected to already know the answer, or even be absolutely 100% certain that you’re correct. You just need to come up with something that would make sense biologically, and is likely to be true.
Example Exam Question
Q6 Paper 1 2023
The question:
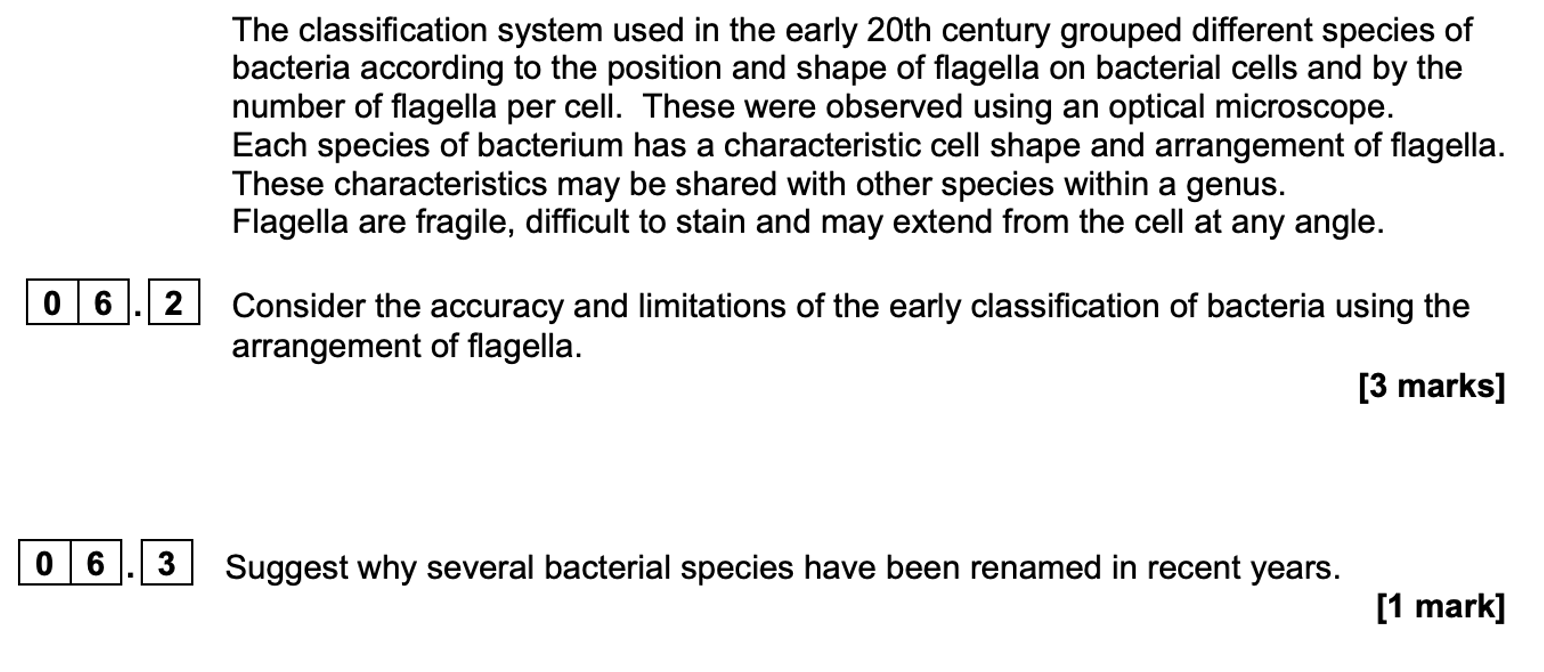
How to approach this question:
1. Don’t panic!
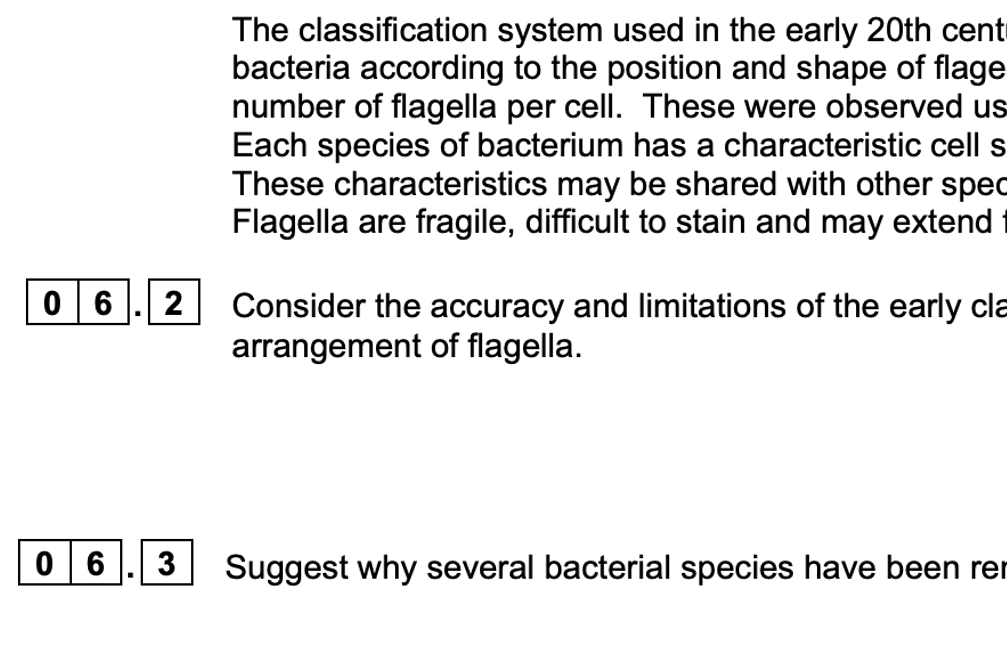
A question about historical classification of bacteria?! That topic is not in the spec!! Don’t panic – all the information you need about any off-spec topic will be provided in the question.
This example question is going to test your knowledge of classification, bacteria and microscopy (all from the spec), and – most crucially - your ability to apply that knowledge in an unfamiliar context.
2. Use your knowledge to make sense of the background information:
You know that bacteria are uni-cellular organisms. Your knowledge of bacterial structure will allow you to understand the description of how bacteria appear under the microscope. You know what a flagellum is. (3.2.1.2)
You know how ‘species’ and ‘genus’ are used in classification (3.4.5)
Your knowledge and experience of microscopy will allow you to understand the description of the limitations of optical microscopes. (3.2.1.3)
3. Answer questions in order
Answering question 6.2 (‘consider’ = ‘review and respond’) first will help you. This question gets you thinking in more detail about things that will help you answer 06.3.
4. Check the Command Word:
Question 6.3 asks you to ‘suggest’. So you know that you should use your existing knowledge/skills to make sense of, and build upon, the information given. You don’t need to know the exact answer for sure, but you need to give a biologically reasonable answer.
5. Understand the question:
The question asks “why” the species have been renamed.
Why might someone rename a species? – because they were misclassified before
Why might they have been misclassified before? – because of the limitations as in your answer to 6.2
Something has changed in recent years that has made it possible to classify these bacteria more accurately than before. What might this be?
6. Think about relevant information from the spec
What have you learned that is related to this question?
Phylogenetic classification (3.4.5)
Methods of studying cells (3.2.1.3)
7. How many marks are there available?
There is only one mark available – you can do this! But if possible, try to include more than one thing that might get a mark, so if one fails you are still ok.
8. So, what’s your answer?
Give it a go before looking at the markscheme below. Remember you need to use specific, technical language to win marks.
…
…
…
…
…
…
Q6 Paper 1 2023 6.3 - mark scheme
A range of answers are acceptable for this 1 mark. How did you do?
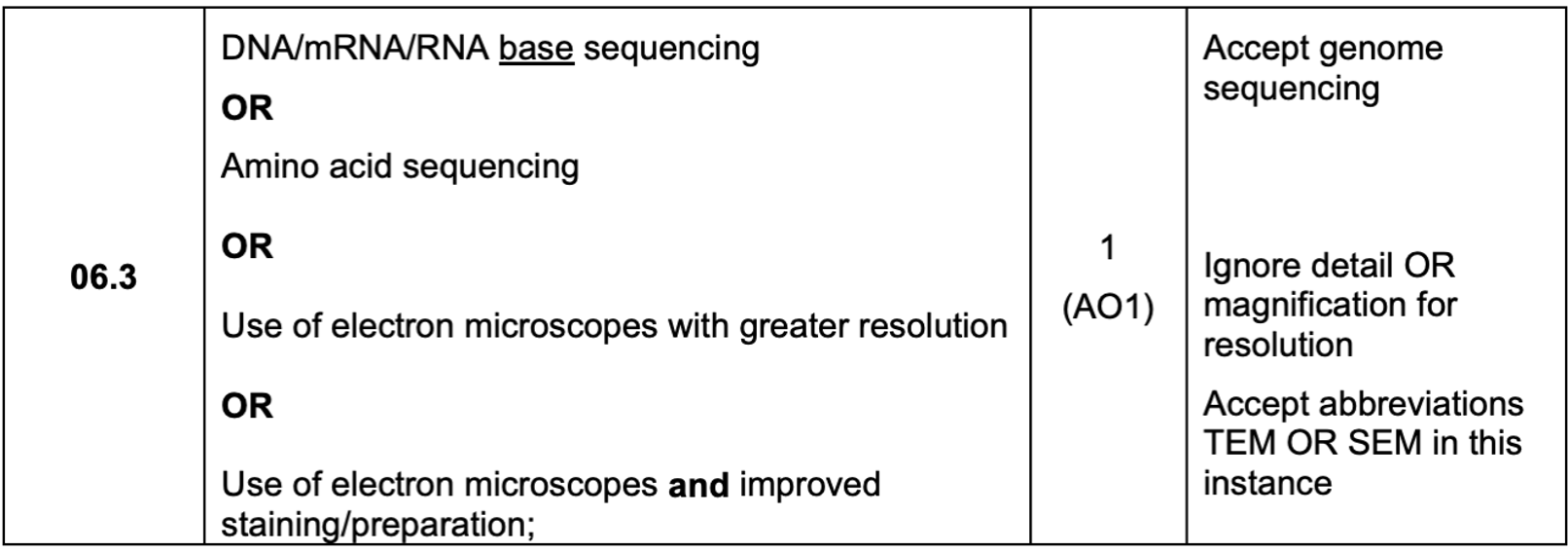
Q6 Paper 1 2023 6.3 – example answers
Successful answer that would win marks:
✅ “Different species will have different DNA sequences so by using genome sequencing they can identify different species”
✅ “Comparing the base sequences of mRNA from the different bacteria will show how similar they are to one another so whether or not they are the same species”
✅ “Electron microscopes have better resolution that optical microscopes so scientists can see the arrangement of the flagella in more detail”
Poor answers that would not get the mark – can you identify where they’ve gone wrong?
❌ “They can identify phylogeny better now, by looking at the DNA”
❌ “They can see more detail with microscopes now so there are fewer mistakes”
❌ “Advanced techniques allow more accurate determination of phylogeny“
A final thought:
The word ‘Suggest’ can be used in different types of questions (e.g. “Suggest two reasons why … ”, “Suggest how … ”) . But the word ‘Suggest’ always invites you to think about the problem in your own way - to use the information in the question with your biology knowledge to come up with your best possible answer.
Want more? Find another “Suggest” exam question walk-through here
Booking now: OCR A Y12 A level Biology Weds 5.15pm from Sept 2026 to June 2027
Weekly Group classes - for OCR A Y12
Raise your exam grade with question focused masterclasses from a highly experienced A level Biology teacher.
Every week we go through a different topic from the specification and look at how to apply the content to exam questions. I show how to understand commonly occurring questions and how to answer them.
Weekly Group classes - for OCR A Y12
Raise your exam grade with question focused masterclasses from a highly experienced A level Biology teacher.
Every week we go through a different topic from the specification and look at how to apply the content to exam questions. I show how to understand commonly occurring questions and how to answer them.
“Outstanding A-level Biology tutoring! Patient, engaging, and highly personalised—even in group classes, it feels one-to-one. Recorded sessions, all questions answered, and every student involved. Our daughter jumped a grade and achieved an A and a place to study Medicine at University” - Google reviews 2025
During the lesson students use an interactive whiteboard to write answers to exam questions which (only) I can see and comment on. Students can ask questions at any time but are not required to speak on camera to the group.
The classes run in focus mode on zoom - so I can see every student, but they are not visible to the rest of the class.
Students can stream a recording of every lesson for revision and note taking.
I teach using evidence-based educational theory. With decades of A level Biology class and one-to-one teaching experience, I am very aware of the misconceptions and misunderstandings that cause students to unnecessarily struggle, and of the mistakes that can lead to dropped marks in exams.
By correcting these issues, students not only do better in exams but also learn to enjoy studying Biology.
The typical class size is 6-12 students. No payment is taken in advance. The classes are £45 per lesson. The card you use to reserve your place is charged after the lesson.
OCR Biology A Y12 Schedule (2026–2027) Time: Wednesdays at 5:15 PM Notes: Closed for Christmas (Dec 23 & 30); Includes sessions during Easter.
| Month | Date | Spec Ref | Topic Focus |
|---|---|---|---|
| September 2026 | 23 Sep | 2.1.1 | Cell structure |
| 30 Sep | 2.1.2 (f) | Water and inorganic ions | |
| October 2026 | 07 Oct | 2.1.2 (a–e) | Microscopy, magnification, and resolution |
| 14 Oct | 2.1.2 (g) | Carbohydrates | |
| 21 Oct | 2.1.2 (h) | Lipids and phospholipids | |
| 28 Oct | 2.1.2 (i) | Proteins | |
| November 2026 | 04 Nov | 2.1.2 (j) | Food tests, colorimetry, calibration, chromatography |
| 11 Nov | 2.1.4 (a–d) | Enzymes and reaction rates | |
| 18 Nov | 2.1.5 (a–b) | Plasma membranes and transport | |
| 25 Nov | 2.1.5 (c), 2.1.4 | Osmosis, enzyme inhibitors, and cofactors | |
| December 2026 | 02 Dec | 2.1.3 (a–c) | Nucleotides and DNA replication |
| 09 Dec | 2.1.3 (d–f) | Protein synthesis | |
| 16 Dec | 2.1.6 (a–e) | Cell cycle and mitosis | |
| 23 Dec | — | No Lesson (Christmas) | |
| 30 Dec | — | No Lesson (Christmas) | |
| January 2027 | 06 Jan | 2.1.6 (f) | Meiosis |
| 13 Jan | 2.1.6 (g) | Cell specialisation and differentiation | |
| 20 Jan | 2.1.6 (h–i) | Stem cells and therapeutic uses | |
| 27 Jan | 3.1.1 (a–b) | Transport in animals – Blood vessels and tissue fluid | |
| February 2027 | 03 Feb | 3.1.1 (c) | The cardiac cycle |
| 10 Feb | Revision | Revision lesson on whole of Module 2 (Practical Qs) | |
| 17 Feb | 3.1.1 (d) | Electrical activity of the heart and ECGs | |
| 24 Feb | 3.1.1 (e) | Carriage of oxygen and carbon dioxide | |
| March 2027 | 03 Mar | 3.1.1 (f) | Foetal/Maternal Haemoglobin and the Bohr shift |
| 10 Mar | 3.1.2 (a–b) | Gas exchange in humans | |
| 17 Mar | 3.1.2 (c) | Gas exchange in plants, insects, fish, and spirometers | |
| 24 Mar | 4.1.1 (a–c) | Communicable diseases – Types and transmission | |
| 31 Mar | 4.1.1 (d–e) | Barriers to infection, inflammation, and phagocytes | |
| April 2027 | 07 Apr | 4.1.1 (f–g) | Specific immune response and antibodies (Easter) |
| 14 Apr | 4.1.1 (h–i) | Immune cell activation and clonal selection (Easter) | |
| 21 Apr | 4.1.1 (j–l) | Immunity, autoimmunity, and vaccination | |
| 28 Apr | 3.1.3 (a–b) | Transport in plants – Xylem and transpiration | |
| May 2027 | 05 May | 3.1.3 (c–e) | Potometers, phloem, xerophytes, and hydrophytes |
| 12 May | 4.2.1 (a–b) | Biodiversity – Levels and sampling | |
| 19 May | 4.2.1 (c–e) | Species richness, Simpson’s Index, genetic diversity | |
| 26 May | 4.2.1 (f–h) | Human impact, agriculture, and conservation | |
| June 2027 | 02 Jun | 4.2.2 (a–c) | Classification and taxonomy |
| 09 Jun | 4.2.2 (d–f) | Evolution and natural selection | |
| 16 Jun | 4.2.2 (h–i) | Adaptations and mechanisms of evolution | |
| 23 Jun | Review | Year 12 Synoptic Review and Practical Skills |
Monoclonal Antibodies in the Immune Response (AQA/OCR, ELISA for AQA)
Monoclonal antibodies are a relatively new treatment type, with huge importance for treating migraine, cancer, autoimmune diseases, and many other conditions.
So how do they work?
What is an Antibody? What is an Antigen?
A guest blog from Dr Jenny Shipway, who studied biochemistry at university and now works in science communication and education training.
Every month, I stab myself in the thigh with an injection pen. It can be painful, but it’s well worthwhile - the pens inject monoclonal antibodies that travel freely in my bloodstream until they reach my head. There, they bind a protein that would otherwise give me migraines. This is the first type of treatment ever designed specifically for migraines. And it’s really, really effective.
Monoclonal antibodies are a relatively new treatment type, with huge importance for treating migraine, cancer, autoimmune diseases, and many other conditions.
So how do they work?
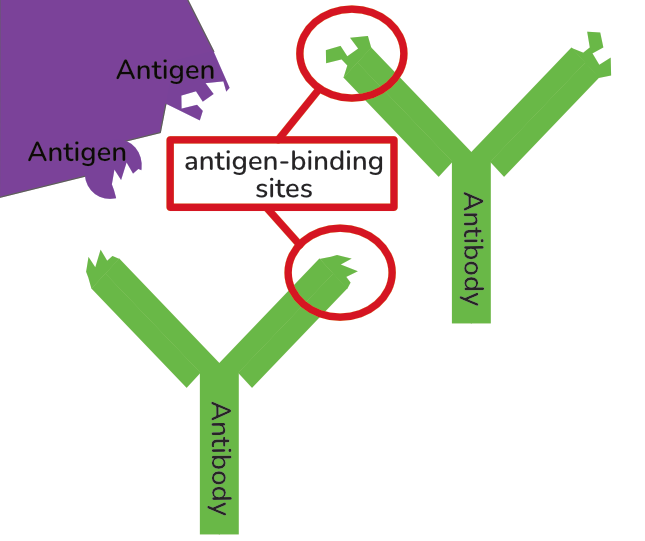
What is an Antibody? What is an Antigen?
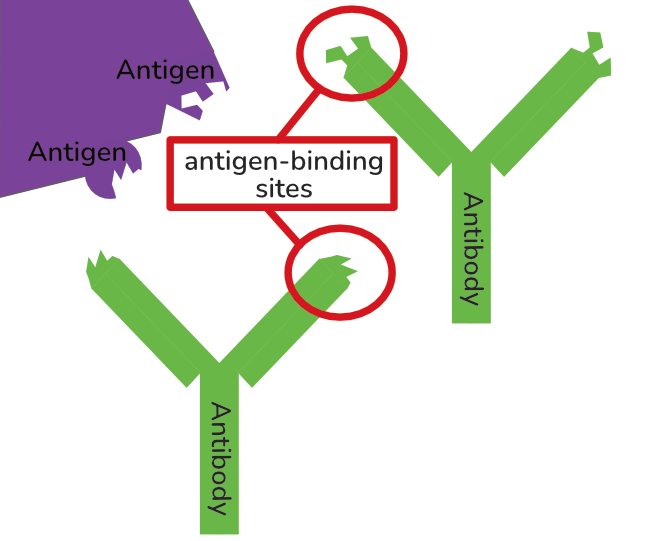
Before you can understand what monoclonal antibodies are, you need a good understanding of antibodies in general. I won’t go through everything here so read this article if you’re not already confident.
To summarise as a recap: antibodies are small protein molecules with variable antigen-binding sites. They bind molecules that don’t belong in the body to flag these up to the immune system. Eg they might bind to a viral surface protein, or a bacterial polysaccharide. The thing that they bind is called an “antigen”.
Monoclonal Antibodies
Mono = one (e.g. monomer, monosaccharide, monoxide)
Clone = an identical copy of a cell/organism with the same DNA, created from one original cell/organism (e.g. clonal selection; clonal expansion; Attack of the Clones)
Antibody = a protein molecule that binds antigens, mediating an immune response
Monoclonal antibodies are identical antibodies, made by B-lymphocytes cloned from one single starter cell.
Why inject Monoclonal Antibodies
Normally, antibodies are synthesised and released in the body by B-lymphocytes. But this requires two things: firstly that the immune system is aware of a threat, and secondly that there is a T-lymphocyte with DNA that encodes the required antibody.
The T-lymphocyte is necessary as it’s involved in sparking off B-lymphocyte replication and antibody production. But also the T-lymphocyte provides a check that it’s safe to use the antibody.
In my case, my body isn’t aware that it would be helpful to make antibodies to that pesky migraine-provoking protein. And I almost certainly don’t have any T-lymphocytes that would give the OK to produce such an antibody. At least, I shouldn’t do. Any such T-lymphocytes should have been destroyed early in my life, along with all other T-lymphocytes that were capable of producing antibodies against my own body. So I need to get the antibodies from somewhere else.
Designer Antigen-Binding Sites
In the lab, you can make any antibody you want. You just need the right B-lymphocyte.
There are a few different ways to tinker with the genetic code of a B-lymphocyte to achieve this. You don’t need to know the details. But what you do need to understand is that inside the B-Lymphoctyle, the scientist needs to ensure that the section of its DNA that codes for the antibody’s antigen-binding site has a sequence that …
… will be translated during protein synthesis into a chain of amino acids which ….
… contains a particular sequence of amino acids (primary structure) so that …
… the chain folds its backbone (secondary structure) in a way that allows …
… the whole thing to fold up upon itself (tertiary structure) so that it …
… presents a binding site with a specific shape and chemical properties that …
… will bind the antigen that they want it to bind.
This one cell can then be cloned. This produces many many identical, cloned cells with that exact same DNA, capable of producing identical antibodies with identical binding sites. Remember mono = one. This is where the “monoclonal” comes from.
Make big vats of these monoclonal cells and you can get them to pump out huge numbers of your chosen antibody to be collected and purified to use as you wish. These are monoclonal antibodies. Each antibody molecule is identical because the cells are all identical clones with the same DNA sequence.
The monoclonal antibodies in my injection pens were made like this in a lab. They have an antigen-binding site that is able to bind a protein called CGRP. By doing so, they prevent the CGRP from binding to its natural receptor, including in a particular set of neurons in my head. Which prevents my migraines.
But monoclonal antibodies can do a lot more than this - they are highly versitile due to their small size and specific binding …
Weaponising Antibodies as Therapeutics
Why stop just with changing the binding site?
Monoclonal antibodies specifically bind to your target, encumbering it and provoking a natural immune response. But why not go further? Why not get the antibody to deliver a powerful weapon directly to its target?
A big problem with injected/ingested drugs is that they get everywhere. If you inject a chemotherapy drug, it travels through the bloodstream without any map or guidance system. It reaches every part of the body. Cancer drugs usually target fast-dividing cells, but this means that as well as damaging the cancer, they get into your hair follicles where they kill healthy cells so that your hair falls out. They get into cells in your gut and kills them, making you feel sick and suffer gastrointestinal problems.
But what if you attached the drug to a monoclonal antibody that only binds the target cancer cells? It will still travel around the body in the blood, but will stop at the cancer and have much greater impact there.
Monoclonal antibodies are used in cancer therapies not only to provoke a normal immune response, but also to deliver cancer drugs, or stick cell-killing radioactive substances onto individual cancer cells. Being able to target the cancer in this way reduces unpleasant side-effects and so broadens the range of drugs that can be used.
Monoclonal Antibodies in Diagnostics
Monoclonal antibodies are useful tools outside the body too.
Until the 1950’s or so, pregnancy tests were carried out using live frogs. They would inject the woman’s urine, and if she was pregnant then her hormones would cause the frog to produce eggs just over a week later. Happily for frogs, we do things a bit differently now. (You don’t need to know about the frogs, although you may now never forget that mental image. You’re welcome.)
The modern pee-on-a-stick pregnancy test is a Lateral Flow Device. They work in very much the same way as Covid tests. You add body fluids, which soak their way along an absorbant strip, and if a certain molecule is present (eg a particular pregnancy hormone, or viral coat proteins) then a visible line appears. How do they detect the molecule of interest? By using monoclonal antibodies that will specifically bind to it. Similar tests can also be used to detect prostate cancer or HIV.
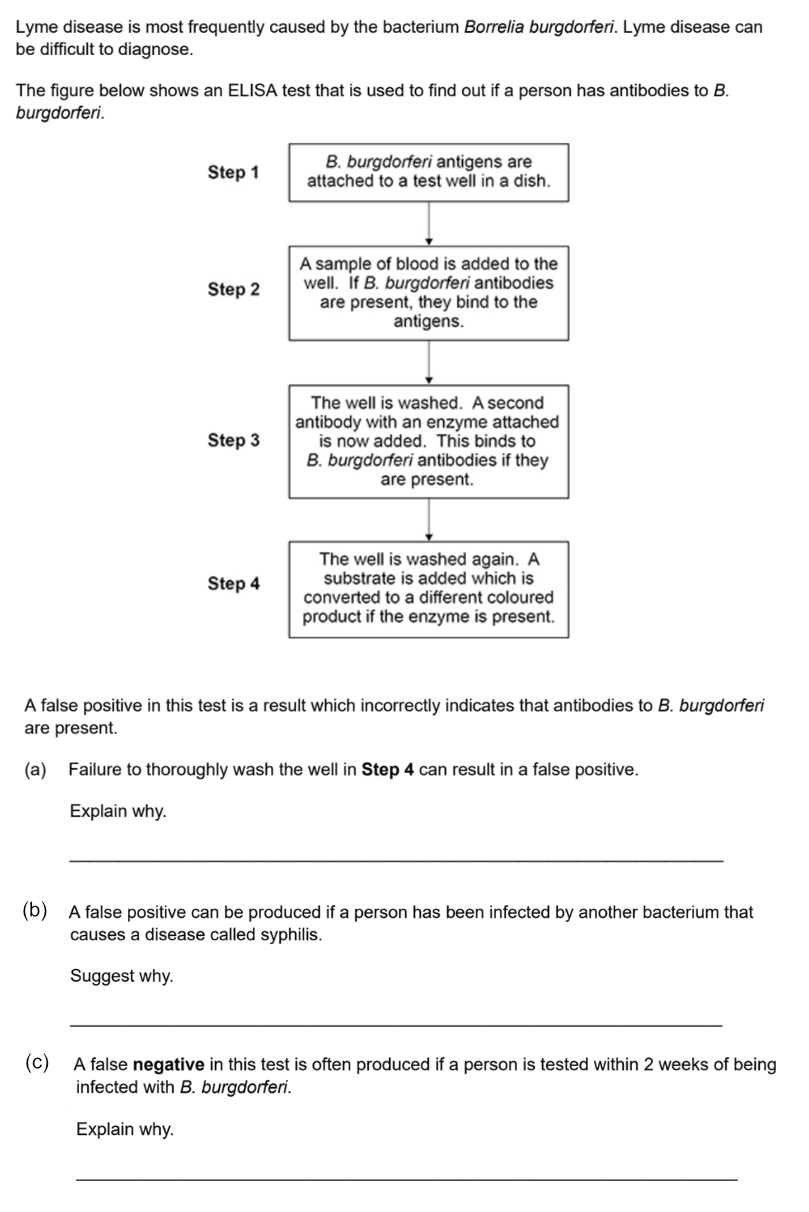
ELISA tests (for AQA)
ELISA tests work in a similar way, biochemically speaking. There are different versions but here’s the one it’s most important to know about. ELISA tests can be confusing because different types of antibodies play different roles in the process.
Direct ELISA test - a test to detect antibodies in the blood
If you are infected with a pathogen, your body will react by producing antibodies that are able to bind antigens associated with that pathogen. By detecting these antibodies, you can be diagnonised as being infected.
Here is how the test works, step by step:
1. An antigen from the pathogen (eg a viral coat protein) is covalently bonded to the well surface.
2. Blood plasma is put into the well. If antibodies for this antigen are present in the blood, they will bind to the antigen.
3. The blood plasma is washed out of the well, leaving behind any antibodies bound to the antigen.
If there are antibodies in the well, then you know the person has had an immune response to the pathogen. But how can you tell if antibodies are there or not? They’re such tiny proteins.
A totally different type of antibody is used for the next step. It’s a monoclonal antibody made in the lab, but it’s also a very unusual one. It is an unnatural, designed tool created purely for use in biochemical assays. These antibodies have some very special properties:
• Their antigen-binding sites specifically bind to the constant region of natural antibodies. This means that for these monoclonal antibodies, other antibodies are antigens! (Yes this is confusing, but it’s a good way to check you really understand what ‘antigen’ means.)
• Their constant region is covalently bonded to an enzyme. The presence of the enzyme means that they can’t bind each others’ constant regions - so they are not antigens to themselves. They only bind other types of antibody.
Imagine the chaos in your body if your B-cells released antibodies that could bind to other antibodies’ constant regions! They would be hugely damaging to your immune system. However, these little guys are very useful tools in the lab.
5. These special monoclonal antibodies, with linked enzyme, are added to the well.
• If there ARE (natural) antibodies bound to the antigen in the well, the monoclonal antibodies will bind to their constant region.
• If there are NO (natural) antibodies, the monoclonal antibodies will remain freely floating in the solvent.
6. The well is washed out again.
The monoclonal antibodies, with their linked enzyme, will only remain in the well IF there were (natural) antibodies in the blood sample. Otherwise they would have been washed away in step 6. If there is enzyme in the well, there must have been antibodies in the blood.
But how do we know if there is enzyme in the well..?! This bit is easy, because of the clever choice of enzyme: The enzyme is one that takes a colourless substrate to form a coloured product.
7. Add the substrate, and see what happens! If colour appears, you know the enzyme is present. And the enzyme if present, its monoclonal antibody must be bound to a natural antibody that could bind the antigen from the pathogen.
AQA Exam Question Example - ELISA tests
This exam question requires you to understand both ELISA tests and the immune response. Can you make sense of it?
Booking now: AQA Y12 A level Biology Group class - from Sept 2026 to June 2027
Weekly Group classes - for AQA Y12 A level Biology
Raise your exam grade with question focused masterclasses from a highly experienced A level Biology teacher.
Every week we go through a different topic from the specification and look at how to apply the content to exam questions. I show how to understand commonly occurring questions and how to answer them.
Weekly Group classes - for AQA Y12 A level Biology
Raise your exam grade with question focused masterclasses from a highly experienced A level Biology teacher.
Every week we go through a different topic from the specification and look at how to apply the content to exam questions. I show how to understand commonly occurring questions and how to answer them.
“Outstanding A-level Biology tutoring! Patient, engaging, and highly personalised—even in group classes, it feels one-to-one. Recorded sessions, all questions answered, and every student involved. Our daughter jumped a grade and achieved an A and a place to study Medicine at University” - Google reviews 2025
During the lesson students use an interactive whiteboard to write answers to exam questions which (only) I can see and comment on. Students can ask questions at any time but are not required to speak on camera to the group.
The classes run in focus mode on zoom - so I can see every student, but they are not visible to the rest of the class.
Students can stream a recording of every lesson for revision and note taking.
I teach using evidence-based educational theory. With decades of A level Biology class and one-to-one teaching experience, I am very aware of the misconceptions and misunderstandings that cause students to unnecessarily struggle, and of the mistakes that can lead to dropped marks in exams.
By correcting these issues, students not only do better in exams but also learn to enjoy studying Biology.
The typical class size is 6-12 students. No payment is taken in advance. The classes are £45 per lesson. The card you use to reserve your place is charged after the lesson.
AQA Biology Y12 Schedule (2026–2027) Time: Tuesdays at 5:15 PM
| Month | Date | Spec Ref | Topic Focus |
|---|---|---|---|
| September 2026 | 29 Sep | 3.2.1.1 | Structure of eukaryotic cells |
| October 2026 | 06 Oct | 3.2.1.2 | Structure of prokaryotic cells and of viruses |
| 13 Oct | 3.2.1.3 | Methods of studying cells | |
| 20 Oct | 3.1.6–8 | Water and inorganic ions | |
| November 2026 | 03 Nov | 3.1.1–2 | Monomers, polymers and carbohydrates |
| 10 Nov | 3.1.3 | Lipids and phospholipids | |
| 17 Nov | 3.1.2–3 | Food tests and calibration curves (applied molecule Qs) | |
| 24 Nov | 3.2.3 | Transport across cell membranes | |
| December 2026 | 01 Dec | 3.2.3 | Osmosis |
| 08 Dec | 3.1.4.1 | General properties of proteins | |
| 15 Dec | 3.1.4.2 | Many proteins are enzymes | |
| January 2027 | 05 Jan | 3.1.5.1, 3.1.6 | Structure of DNA and RNA, ATP |
| 12 Jan | 3.1.5.2 | DNA replication | |
| 19 Jan | 3.2.2 | All cells arise from other cells | |
| 26 Jan | 3.2.4 | Cell recognition and the immune system | |
| February 2027 | 02 Feb | 3.2.4 | HIV and monoclonal antibodies |
| 09 Feb | 3.3.1, 3.3.2 | SA:V, gas exchange in insects and fish | |
| 16 Feb | Revision | Revision lesson on 3.1 and part of 3.2 | |
| 23 Feb | 3.3.2 | Gas exchange in humans | |
| March 2027 | 02 Mar | 3.3.3 | Digestion and absorption |
| 09 Mar | 3.3.4.1 | Mass transport in animals – Circulatory system & tissue fluid | |
| 16 Mar | 3.3.4.1 | The heart and cardiac cycle | |
| 23 Mar | 3.3.4.1 | Haemoglobin and the Bohr shift | |
| April 2027 | 13 Apr | 3.3.4.2 | Mass transport in plants – Xylem and potometers |
| 20 Apr | 3.3.4.2 | Phloem – Mass flow hypothesis | |
| 27 Apr | 3.4.1 | DNA, genes and chromosomes | |
| May 2027 | 04 May | 3.4.2 | DNA and protein synthesis |
| 11 May | 3.4.3 | Genetic diversity – mutations and meiosis | |
| 18 May | 3.4.4 | Genetic diversity and adaptation | |
| ``` |
AQA Paper 3 Extended Essay: Tips, Mark Scheme and Past Paper Titles - Updated for 2026
How to answer the AQA A-level Biology Extended Essay, including past paper essay titles
Exam Boards give feedback about students’ answers each year, to help future students do better. I have been working with some tutees, using the examiners’ guidance, to improve their approach to the AQA Paper 3 Extended Essay.
What are Extended Essays

The synoptic essay question is found at the end of AQA A-Level Biology Paper 3. You are required to write, in sentences and paragaphs of text, an essay about one of two topics. You should plan to spend about 40 minutes on the essay.
E.g.: “Write an essay on using DNA in science and technology”, or “Write an essay on the importance of membranes in the functioning of cells”.
In your essay you must write about a central theme, bringing together different ideas and concepts from the specification.
Why is there an Essay in the Paper?
Examiners want to check that you understand how different topic areas relate to bigger themes – how and why they are important in different contexts. This requires a deeper understanding of the topics.
You are tested on your ability to pick appropriate topics to write about, and your ability to present these using A-level terminology in a way that highlights their connection to the central theme.
Mark Scheme
There are 25 marks available for the essay, but remember you don’t need all of them to get a top grade. Even for an A* it’s ok to aim for 18/25.
Essays are assessed within ‘levels of response’, with each level having different marks available. See the table below, where each row is a different level. You need to meet a variety of measures to reach each level.
The qualities examiners look for are:
How well you link the topic areas to the main theme
A-level standard material with appropriate terminology, clearly explained
Avoiding factual errors
Avoiding irrelevant topics/information
Notice that because of the way the marking works, there’s no point in doing one thing incredibly well while ignoring the others. The things you do badly would hold you back from advancing through the levels.
Examiners’ Mark Scheme (marks for each level are shown in the left-hand column):
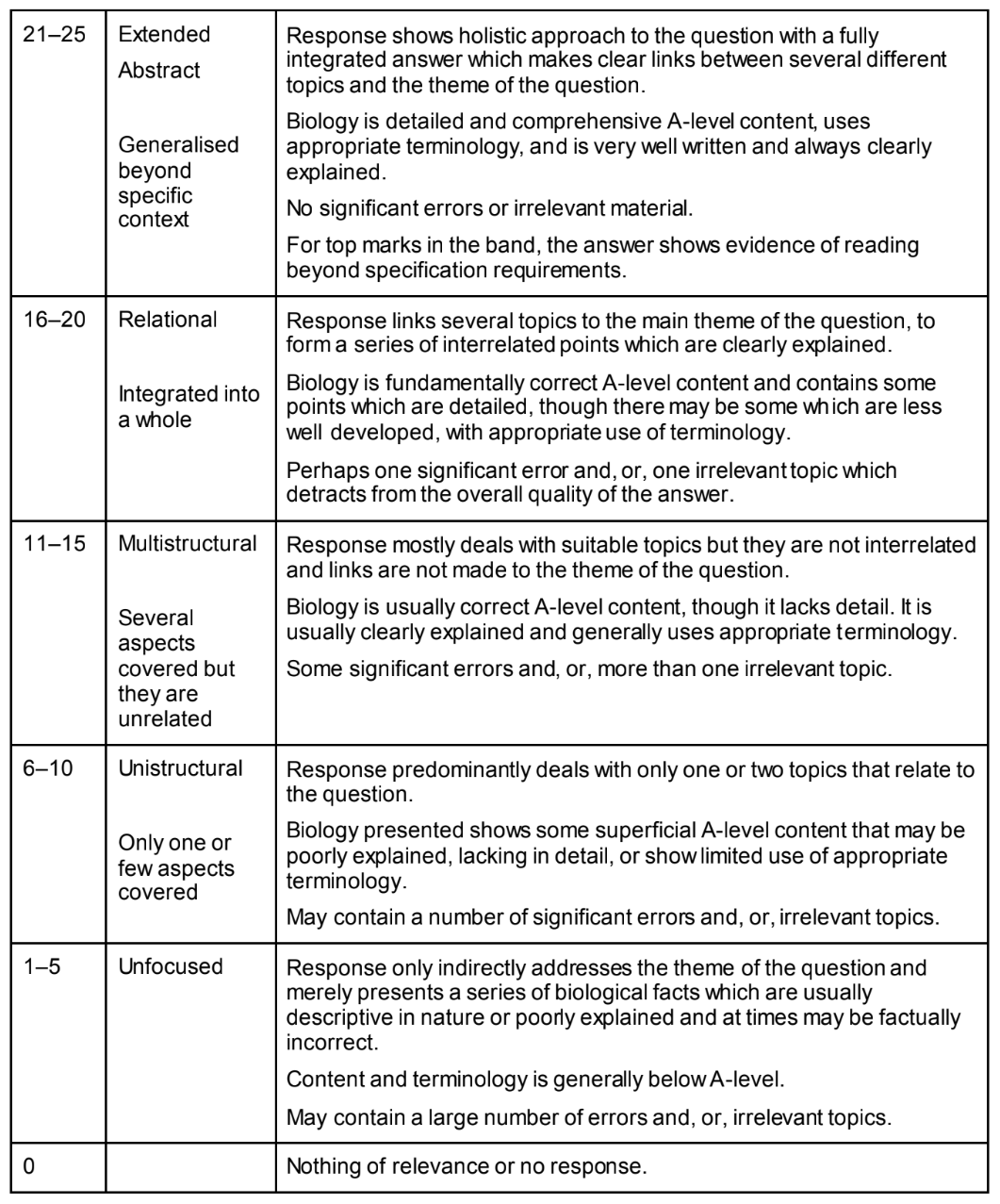
Selecting Topic Areas
You must identify an underlying theme or idea in the essay title – this must be a ‘big idea’ that you can illustrate in different ways.
You then need to choose ‘several’ topic areas that you can relate to this theme.
A ‘topic area’ is a numbered sub-section in the specification
Topic areas should be as different as possible from each other
AQA say you should have a minimum 4 topic areas.
I suggest you aim for 5 or 6 topic areas.
Picking topic areas can be a challenge. Here’s my top tip for how to approach this:
Think your way through the Kingdoms of Life. Can you think of illustrative examples from each Kingdom? (Ok, maybe not protists.)
Think your way through different scales. From single molecules → macromolecule → organelle → cells → tissue → organ → organ system → individual → populations → community → ecosystem.
Picking topic areas using this technique should give you both breadth and depth.
Want more? See this article all about picking topic areas, including a list of past-paper titles and examiners’ guidance.
A note on off-spec topics: to score 24 or 25/25, you would need to include a topic outside the A-level specification. But I always recommend students stay within spec. You don’t need 24/25 to get an A* overall (18/25 is fine), and many students attempting off-spec topics fail due to lack of depth and scientific terminology. Using something you heard in a podcast isn’t enough; you need to present it at or above A-level standard. Of course it’s great if you can! But only attempt this if extremely confident as else it could reduce your overall marks.
How to Structure your Essay
Writing an essay plan might be useful if it doesn’t take too long. But remember you will only get marks for content that is presented in sentences/paragraphs within the actual essay.
Overview:
Write in full sentences/paragraphs – you will only gets marks for things presented in this way.
No introduction or conclusion – Examiners say these are a waste of your time
Separate sections for each of your chosen topic areas – they don’t need to link to each other
Avoid diagrams – you will only get marks for things described in writing.
For each topic area, you need to:
Present information about a relevant concept/idea from the topic area, using A-level detail and terminology. You need most of your essay to reach A-level standard if you are to get more than 10 marks.
Explain how and why the chosen concept/idea relates to the central theme. Why is it relevant and/or important. Without doing this, it is impossible to get more than 15 marks.
What Topic Information to Include
Content must be of A-level standard to score well – this includes information, terminology, and the explanation of ‘importance’ to the theme.
Don’t just splurge out everything you can remember. Only include things where you can also explain how the given information relates to the theme and why it is important.
Don’t let one or two topic areas dominate the essay - share your time between them. If one of your topic areas is large, and/or one that you know in depth, just pick the more relevant/important parts.
Don’t add extra bonus bits of information just because you can! Adding irrelevant information can prevent you reaching the next level, losing you marks.
Watch your Language – style and terminology
This isn’t an English exam; there are no points for style or narrative. Just get the important information down as clearly and concisely as possible. Short sentences are best for clarity. (But no bullet points; the examiners only mark full sentences.)
Crucially, you need to use precise, very scientific, A-level language appropriate to this level of study. Say exactly what you mean at all time. State units, and give the correct scientific names of molecules, bonds, processes etc.
Avoid ambiguous and non-specific language. Never use words like level, amount, nutrient, enables, supports, signals, messages, size, breaks down, or encourages. Many students lose marks from using these words in place of correct terminology.
Examiners reported: “Appropriate terminology was often poorly used or absent. For example, many students wrote about ‘signals’ and ‘messages’ rather than impulses/action potentials. The use of ‘levels’ and ‘amounts’ for concentration was also very common.”
Example Essay
Here is an example essay that scored 18/25. That’s a good quality for most people to be aiming for. It has some annotations from the examiner showing how they responded to the work.
If you want to have a go writing your own essay on this theme first, to compare approaches, it’s “Write An Essay On The importance of nitrogen-containing substances in biological systems”. Remember there are many different ways to approach these essays, so if you pick different topic areas that isn’t anything to worry about. But how do your information and terminology and thematic links compare?
For topic areas, go to “picking topic areas, past paper titles, and examiners’ guidance” which lists topic areas suitable for these titles, and more about how to approach choosing your topics.
Phosphorus-containing substances and their importance in biological systems.
The mechanisms and importance of transport within organisms.
The importance of interactions between organisms and their environment.
The importance of shapes fitting together in cells and organisms.
How bacteria can affect the lives of humans and other organisms.
A cycle is a biological pathway or process in which the end product of one cycle becomes the starting point for the next cycle. Write an essay on cycles in biology.
Carbon dioxide may affect organisms directly or indirectly. Write an essay to describe and explain these effects.
Polymers have different structures. They also have different functions. Write an essay to describe how the structures of different polymers are related to their functions.
Using DNA in science and technology.
The importance of membranes in the functioning of cells.
More AQA Paper 3 Extended Essay Titles (older)
If you found it useful then please ❤️ (at the bottom of the page) and share
I run weekly AQA specific group classes for Y12 and Y13 students - details here

Example AQA Paper 3 Extended Essay
This is an example essay published by AQA as guidance. It scored 18/25 which is a good level for most students to be aiming at. Could you write at this standard? Can you see where they could have done better? Did they need to write so much to get these marks?
This is an example essay published by AQA as guidance. It scored 18/25 which is a good level for most students to be aiming at. Could you write at this standard? Can you see where they could have done better? Did they need to write so much to get these marks?
See the Extended Essay mark scheme here
Write An Essay On The importance of nitrogen-containing substances in biological systems